AORTIC DISSECTION
1. Establish large bore IV access and titrate FiO2 to SpO2 ≥ 90%.
2. Place right radial arterial line and use left arm for NIBP.
3. Use fentanyl and esmolol as first line therapy to control pain, keep HR < 60 and reduce SBP < 120 mmHg.
4. If additional control is needed, use the agents listed (in order of preference) in the table opposite.
5. Prepare for rapid CT angiogram but use bedside TEE or TTE as alternatives if unstable or while waiting for CT.
6. Notify blood bank, request blood products and activate massive transfusion protocol if indicated .
7. Seek early consultation with CT surgeon for decision on imaging, blood pressure, and heart rate control.
8. Notify theatre early if surgery is indicated.
9. If hypotensive, consider tamponade, myocardial infarction, aortic valve incompetence or aortic rupture.
10. Prepare for transfer to ICU or the OR.
Principles are to control BP, stop bleeding and replace volume. Morbidity and mortality is directly proportional to the delay in diagnosis and management. Early placement of arterial line for monitoring and sampling helps guide treatment.
Dissection progression and mortality is proportional to flow velocity and pressure differentials (dP/dT) so decrease HR, inotropy and SBP
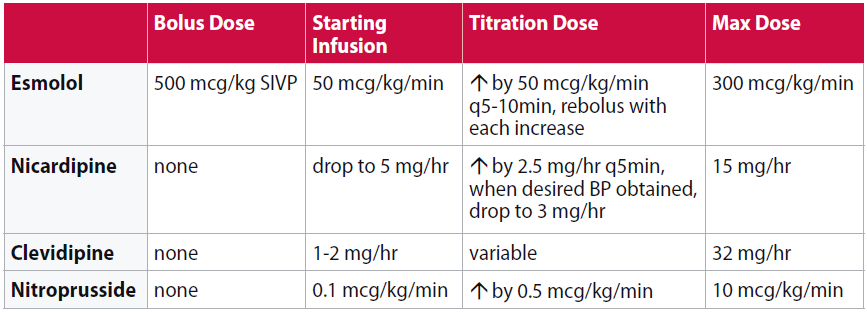
If the above are unavailable, consider metoprolol or diltiazem for HR and labetalol for additional BP control.
Rapid imaging options
CTA chest/abdomen ± neck or lower extremities.
TEE/TTE if unstable or awaiting CT scanner.
CTA (CT with arterial contrast) is generally the most available imaging modality with similar accuracy to TEE and MRA. Bedside TTE, aortic, or carotid imaging are available rapid adjuncts to make the diagnosis and begin focused management but are not sufficiently sensitive to exclude dissection.
Hypotension may be due to myocardial infarction, aortic incompetence, tamponade or aortic rupture. Use ECG and bedside echo to look for treatable causes.
Thoracic aortic dissection is a rare but lethal disease (3.5/100000). Only 85% of patients present with a sudden onset of severe pain. Beware patients who have sudden symptoms involving disparate anatomical systems, or chest pain plus other symptomatology and have a low threshold for investigating further.