News, Guidelines, Tips & Tricks for doctors, anesthesiologists, cardiac anesthesiologists, and intensive care specialists.
Experts’ guidelines of intubation and extubation of the ICU patient
Get link
Facebook
X
Pinterest
Email
Other Apps
French Society of Anaesthesia and Intensive Care Medicine (SFAR) and French-speaking Intensive Care Society (SRLF)
In collaboration with the pediatric Association of French-speaking Anaesthetists and Intensivists (ADARPEF), French-speaking Group of Intensive Care and Paediatric emergencies (GFRUP) and Intensive Care physiotherapy society (SKR) Hervé QuintardEmail author, Erwan l’Her, Julien Pottecher, Frédéric Adnet, Jean-Michel Constantin, Audrey De Jong, Pierre Diemunsch, Rose Fesseau, Anne Freynet, Christophe Girault, Christophe Guitton, Yann Hamonic, Eric Maury, Armand Mekontso-Dessap, Fabrice Michel, Paul Nolent, Sébastien Perbet, Gwenael Prat, Antoine Roquilly, Karim Tazarourte, Nicolas Terzi, Arnaud W. Thille, Mikael Alves, Etienne Gayat and Laurence Donetti Annals of Intensive Care2019
Abstract Background Intubation and extubation of ventilated patients are not risk-free procedures in the intensive care unit (ICU) and can be associated with morbidity and mortality. Intubation in the ICU is frequently required in emergency situations for patients with an unstable cardiovascular or respiratory system. Under these circumstances, it is a high-risk procedure with life-threatening complications (20–50%). Moreover, technical problems can also give rise to complications and several new techniques, such as videolaryngoscopy, have been developed recently. Another risk period is extubation, which fails in approximately 10% of cases and is associated with a poor prognosis. A better understanding of the cause of failure is essential to improve success procedure.
Results and conclusion In constructing these guidelines, the SFAR/SRLF experts have made use of new data on intubation and extubation in the ICU from the last decade to update existing procedures, incorporate more recent advances and propose algorithms. Introduction
Intubation and extubation of ventilated patients are not risk-free procedures on the intensive care unit (ICU) and can be associated with morbidity and mortality. Intubation in the ICU is frequently required in emergency situations for patients with an unstable cardiovascular system who may be hypoxic [1, 2, 3]. Under these circumstances it is a high-risk procedure with life-threatening complications (20–50%) such as hypotension and respiratory failure [2]. Technical problems can also give rise to complications. Generally three unsuccessful intubations [4] or two unsuccessful attempts at laryngoscopy are needed to justify the description difficult airway. These can make up 10–20% of intubations in the ICU and are associated with an increase in morbidity [2]. Several new techniques such as videolaryngoscopy have been developed for difficult airway management, but contrary to operating room practice, integrating these into ICU algorithms is not well established.
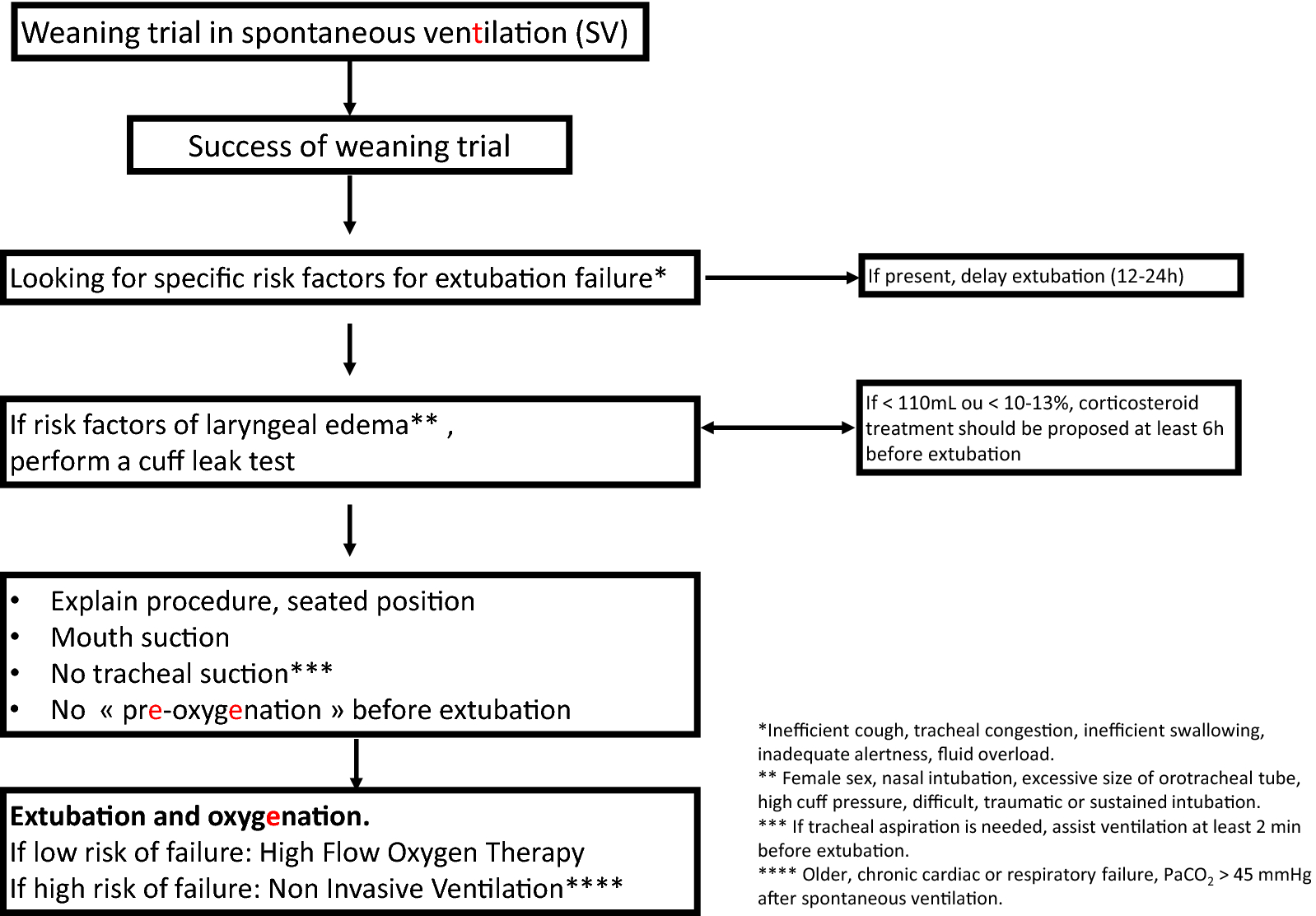
Another period of risk is extubation, which fails in approximately 10% and is associated with a poor prognosis [5, 6]. Extubation follows the successful weaning of patients from mechanical ventilation [7, 8, 9], but sometimes the re-establishment of spontaneous breathing is only possible with the tube in situ. An extubation failure is defined as the need for reintubation within 48 h of tube removal [7, 10], and the most recent consensus on weaning defined success as an absence of mechanical assistance for 48 h after extubation. There is a need to incorporate into these definitions the development of noninvasive ventilation (NIV) after extubation. NIV can be used as a weaning aid during extubation or as a preventive or curative treatment in acute respiratory failure occurring after extubation [11, 12]. As NIV can postpone the need for reintubation, a period of 7 days after extubation is required for a more accurate definition of failure [12]. To reduce the incidence of failure to extubate, the role of pathologies such as swelling and laryngeal edema in increasing risk must be appreciated. Screening for risk factors that might predispose to failure to extubate could improve the chances of success. In constructing these guidelines we have made use of new data on intubation and extubation in the ICU from the last decade to update existing procedures and incorporate more recent advances.
Materials and methods
Table 1 represents a total of 19 experts were separated into 7 working groups (the pediatric experts being involved in all questions): The management of intubation has been assessed according to four headings: complicated intubation in the ICU, the materials required, pharmacology and the use of a management protocol. Extubation has been assessed according to three headings: prerequisites for extubation, extubation failure and the use of a management protocol. A specific analysis was performed for intubation and extubation in children.
Table 1
Guideline timeline
September 9, 2015
Start-up meeting
February 2016
Vote: first round
February 24, 2016
Postvote deliberation meeting
March 21, 2016
Vote: second round
June 2016
Amendment of two guidelines
September 2016
Guideline finalization meeting
As a first step, the organization committee defined the questions under consideration according to the PICO format (Patients Intervention Comparison Outcome). The system used to elaborate their recommendations is the GRADE® method [13, 14].
These guidelines with their arguments were published in the journal Anaesthesia Critical Care and Pain Medicine [15, 16].
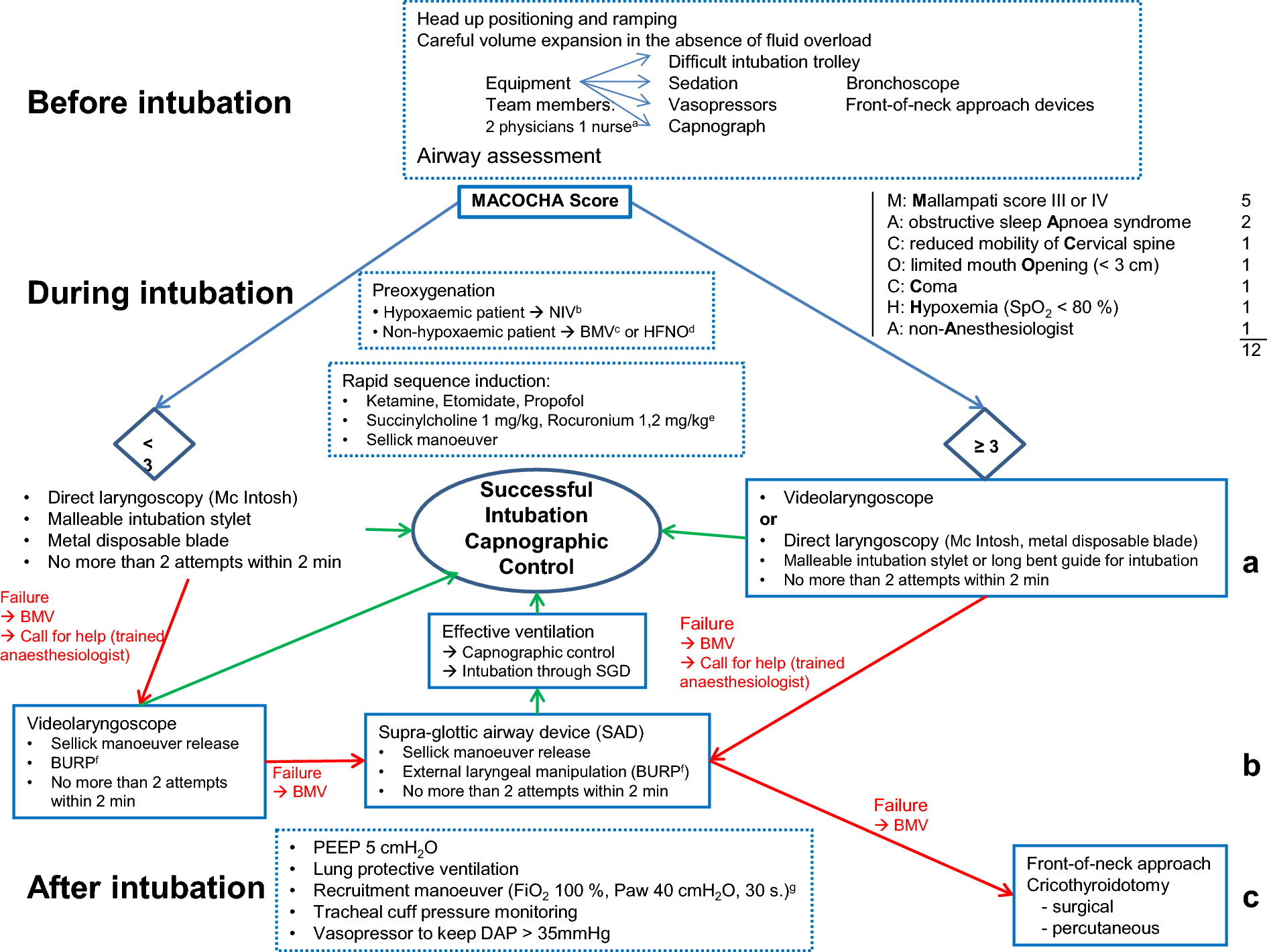
Fig. 1
Algorithm for intubation
Fig. 2
Algorithm for extubation
Intubation of the ICU patient (Fig. 1 )
Complicated intubation in ICU
R 1.1—All patients admitted to intensive care units must be considered at risk of complicated intubation. (Grade 1 +) Strong agreement.
R 1.2—To reduce the incidence of complicated intubation, respiratory and haemodynamic complications must be anticipated and prevented, by careful preparing for intubation, and taking steps to maintain oxygenation and cardiovascular stability throughout the procedure. (Grade 1 +) Strong agreement.
R 1.3—Risk factors of complicated intubation must be distinguished from predictive factors of difficult intubation. (Grade 1 +) Strong agreement.
Intubation equipment
R 2.1—Capnographic control of intubation in the intensive care environment is necessary to confirm the correct position of the endotracheal tube, the supraglottic device or the direct approach through the trachea. (Grade 1 +). Strong agreement.
R 2.2—It is necessary to have a Difficult Airway Trolley and a Bronchoscope (conventional or single use) in intensive care units, for the immediate management of difficult intubation. (Grade 1 +) Strong agreement.
R 2.3—Metal blades should be used for direct laryngoscopy in ICU to improve the success rate of endotracheal intubation. (Grade 1 +) Strong agreement.
R 2.4—In order to limit intubation failures, videolaryngoscopes (VL) for intubation in intensive care must be used either initially or after failure of direct laryngoscopy. (Grade 2 +) Strong agreement.
R 2.5—Supraglottic devices (SGD) must be used in the management of difficult intubation in intensive care, to oxygenate the patient, and facilitate intubation under bronchoscopic control. (Grade 1 +) Strong agreement.
R 2.6—Theoretical and practical intubation knowledge must be acquired and diligently maintained (Grade 1 +) Strong agreement.
Drugs and intubation of the ICU patient
R 3.1—A hypnotic agent that facilitates rapid sequence induction (RSI) should probably be used (Etomidate, Ketamine, Propofol), the choice depending on medical history and the clinical situation of the patient. (Grade 2 +) Strong agreement.
R 3.2—In critically ill patients, to facilitate tracheal intubation during RSI (rapid sequence induction), succinylcholine use is probably recommended (Grade 2 +) Strong agreement.
R 3.3—Rocuronium at a dose above 0.9 mg/kg [1.0–1.2 mg/kg] should be used when succinylcholine is contraindicated. (Grade 1 +) Sugammadex should probably be rapidly available when rocuronium is used (Grade 2 +) Strong agreement.
Protocols, algorithms and intubation of the ICU patient
R 4.1—Non-invasive ventilation should probably be used for pre-oxygenation of hypoxaemic patients in ICU. (Grade 2 +) Strong agreement.
R 4.2—It is possible to use high-flow nasal oxygen (HFNO) for pre-oxygenation in ICU, especially for patients not severely hypoxaemic. (Expert opinion) Strong agreement.
R 4.3—A protocol for intubation including a respiratory component should probably be used in ICU to decrease respiratory complications. (Grade 2 +) Strong agreement.
R 4.4—A post-intubation recruitment manoeuvre should probably be used in ICU in hypoxaemic patients, by integrating it into the respiratory component. (Grade 2 +) Strong agreement.
R 4.5—A PEEP of at least 5 cmH2O should probably be applied after intubation of hypoxaemic patients. (Grade 2 +) Strong agreement.
R 4.6—A cardiovascular component should probably be included in the protocol during intubation of ICU patients, by defining conditions of fluid challenge and early administration of amines to decrease cardiovascular complications. (Grade 2 +) Strong agreement.
In the high-stakes environment of the OR and the ICU, time is the ultimate variable. When a patient develops acute respiratory failure, waiting for a portable X-ray or transporting a hemodynamically unstable patient to CT can be risky, if not impossible. Enter the BLUE Protocol (Bedside Lung Ultrasound in Emergency) . Developed by Professor Daniel Lichtenstein, this diagnostic algorithm allows an anesthesiologist to identify the cause of dyspnea with over 90% accuracy in under 3 minutes. What is the BLUE Protocol? The BLUE Protocol is a standardized ultrasound algorithm designed for the rapid differential diagnosis of acute respiratory distress. By focusing on specific artifacts rather than traditional imaging, it provides immediate clinical answers. Standardized Scanning: The BLUE-Points To ensure reproducibility—much like the six leads of an ECG—the BLUE-protocol utilizes six standardized points (three on each side) that maximize lung coverage while avoiding the heart:
The WHO Surgical Safety Checklist keywords:WHO Surgical Safety Checklist, surgical safety, patient safety, operating room protocols, perioperative care, checklist implementation, surgical errors, teamwork in surgery, anesthesia safety, infection prevention, surgical complications The World Health Organization Surgical Safety Checklist establishes protocols designed to prevent the occasional, but recurring errors that have led to harm. The Safety Checklist applies from the time before induction of anesthesia, through just before skin incision and on to the time before the patient leaves the operating room.
Tricks how to hit a vein every time venipuncture, how to hit a vein, IV insertion, vein access tricks, intravenous therapy, hitting a vein every time, vein finder, anesthesiology tips, myocardial protection, difficult veins, IV catheter placement, vein dilation, tourniquet technique, phlebotomy skills, needle insertion . Choosing the Catheter Gauge depends on the clinical scenario: