Practice Advisory for Intraoperative Awareness and Brain Function Monitoring: A Report by the American Society of Anesthesiologists Task Force on Intraoperative Awareness
PRACTICE advisories are systematically developed reports that are intended to assist decision making in areas of patient care. Advisories provide a synthesis and analysis of expert opinion, clinical feasibility data, open forum commentary, and consensus surveys. Advisories are not intended as standards, guidelines, or absolute requirements. They may be adopted, modified, or rejected according to clinical needs and constraints.
The use of practice advisories cannot guarantee any specific outcome. Practice advisories summarize the state of the literature and report opinions derived from a synthesis of task force members, expert consultants, open forums, and public commentary. Practice advisories are not supported by scientific literature to the same degree as are standards or guidelines because sufficient numbers of adequately controlled studies are lacking. Practice advisories are subject to periodic revision as warranted by the evolution of medical knowledge, technology, and practice.
Methodology
A. Definitions
Intraoperative awareness under general anesthesia is a rare occurrence, with a reported incidence of 0.1–0.2%.1–4 Significant psychological sequelae (e.g. , post–traumatic stress disorder) may occur after an episode of intraoperative awareness, and affected patients may remain severely disabled for extended periods of time.5 However, in some circumstances, intraoperative awareness may be unavoidable to achieve other critically important anesthetic goals.
The following terms or concepts discussed in this Advisory include: consciousness, general anesthesia, depth of anesthesia or depth of hypnosis, recall, amnesia, intraoperative awareness, and brain function monitors. Consistent definitions for these terms are not available in the literature. For purposes of this Advisory, these terms are operationally defined or identified as follows:
1. Consciousness.
Consciousness is a state in which a patient is able to process information from his or her surroundings. Consciousness is assessed by observing a patient’s purposeful responses to various stimuli. Identifiers of purposeful responses include organized movements following voice commands or noxious/painful stimuli.1For example, opening of the eyes is one of several possible identifiers or markers of consciousness. Purposeful responses may be absent when paralysis is present as a consequence of neurologic disease or the administration of a neuromuscular blocking drug.
2. General Anesthesia.
General anesthesia is defined as a drug-induced loss of consciousness during which patients are not arousable, even by painful stimulation.2The ability to maintain ventilatory function independently is often impaired. Patients often require assistance in maintaining a patent airway, and positive-pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired.
3. Depth of Anesthesia.
Depth of anesthesia or depth of hypnosis refers to a continuum of progressive central nervous system depression and decreased responsiveness to stimulation.
4. Recall.
For the purpose of this Advisory, recall is the patient’s ability to retrieve stored memories. Recall is assessed by a patient’s report of previous events, in particular, events that occurred during general anesthesia. Explicit memory is assessed by the patient’s ability to recall specific events that took place during general anesthesia. Implicit memory is assessed by changes in performance or behavior without the ability to recall specific events that took place during general anesthesia that led to those changes.6 A report of recall may be spontaneous or it may only be elicited in a structured interview or questionnaire. This Advisory does not address implicit memory.
5. Amnesia.
Amnesia is the absence of recall. Many anesthetic drugs produce amnesia at concentrations well below those necessary for suppression of consciousness. Anterograde amnesia is intended when a drug with amnestic properties is administered before induction of anesthesia. Retrograde amnesia is intended when a drug such as a benzodiazepine is administered after an event that may have caused or been associated with intraoperative consciousness in the hope that it will suppress memory formation and “rescue” from recall.
6. Intraoperative Awareness.
Intraoperative awareness occurs when a patient becomes conscious during a procedure performed under general anesthesia and subsequently has recall of these events. For the purpose of this Advisory, recall is limited to explicit memory and does not include the time before general anesthesia is fully induced or the time of emergence from general anesthesia, when arousal and return of consciousness are intended. Dreaming is not considered intraoperative awareness.
7. Brain Function Monitors.
Brain function monitors are devices that record or process brain electrical activity and convert these signals mathematically into a continuous measure typically scaled from 0 to 100. In addition to monitoring spontaneous cortical electrical activity (electroencephalogram [EEG]), these devices may also record and process evoked cortical and subcortical activity (auditory evoked potentials [AEPs]) as well as electromyographic (EMG) activity from scalp muscles. For the purpose of this Advisory, only monitors purported to measure depth of anesthesia or hypnosis will be considered. Other, non-EEG, non-AEP, non-EMG devices are also available but are not addressed by this Advisory.
B. Purposes of the Advisory
Intraoperative awareness under general anesthesia is an important clinical problem that clearly is within the foundation of training and continuing medical education in anesthesiology. The purposes of this Advisory are to identify risk factors that may be associated with intraoperative awareness, provide decision tools that may enable the clinician to reduce the frequency of unintended intraoperative awareness, stimulate the pursuit and evaluation of strategies that may prevent or reduce the frequency of intraoperative awareness, and provide guidance for the intraoperative use of brain function monitors as they relate to intraoperative awareness.
C. Focus
This Advisory focuses on the perioperative treatment of patients who are undergoing a procedure during which general anesthesia is administered. This Advisory is not intended for the perioperative management of minimal, moderate, or deep sedation in the operating room or intensive care unit; regional or local anesthesia without general anesthesia; monitored anesthesia care; tracheal intubation of patients or those undergoing resuscitation in emergency trauma after the administration of a neuromuscular block, or intentional intraoperative wake-up testing (e.g. , for the purposes of assessing intraoperative neurologic function). In addition, this Advisory is not intended to address the perioperative treatment of pediatric patients.
D. Application
This Advisory is intended for use by anesthesiologists, other physicians who supervise the administration of general anesthesia, and all other individuals who administer general anesthesia. The Advisory may also serve as a resource for other physicians and healthcare professionals who are involved in the perioperative management of patients receiving general anesthesia.
E. Task Force Members and Consultants
The American Society of Anesthesiologists (ASA) appointed this Task Force of 10 members to (1) review and assess the currently available scientific literature on intraoperative awareness, (2) obtain expert consensus and public opinion, and (3) develop a practice advisory. The Task Force is comprised of anesthesiologists from various geographic areas of the United States, an anesthesiologist from The Netherlands, and two methodologists from the ASA Committee on Practice Parameters.
The ASA appointed the 10 members to the Task Force because of their knowledge or expertise in the medical specialty of anesthesiology, and the development of practice parameters. The members include but are not limited to anesthesiologists with specialized knowledge or expertise in the area of neuroanesthesiology. Two of the 10 members disclosed receipt of funds from or a financial interest in a company developing or manufacturing brain function monitors; these companies have a direct financial interest in the expanded use of such monitors. Task Force members may also have received funds from or have a financial interest in other companies, such as developers or manufacturers of anesthetics, that may be indirectly affected by the expanded use of brain function monitors. The Task Force did not request for its members to disclose such interests because they were deemed too remote and speculative to present conflicts of interest.
The Task Force, in turn, sought input from consultants, many of whom who had particularized knowledge, expertise, and/or interest in intraoperative awareness and brain function monitors. Such knowledge or expertise is based in part in some cases on research or investigational activities funded by a company developing or manufacturing brain function monitors. Fifty-four percent of the consultants disclosed receipt of funds from or a financial interest in a company developing or manufacturing brain function monitors. Consultants also may have received funds from or have a financial interest in other companies that may be indirectly affected by the use of brain function monitors. The Task Force did not request for its consultants to disclose such interests because they were deemed too remote and speculative to present conflicts of interest.
The Task Force used a six-step process. First, the members reached consensus on the criteria for evidence of effective perioperative interventions for the prevention of intraoperative awareness. Second, they evaluated original articles published in peer-reviewed journals relevant to this issue. Third, consultants who had expertise or interest in intraoperative awareness and who practiced or worked in diverse settings (e.g. , scientists and/or physicians in academic and private practice) were asked to participate in opinion surveys on the effectiveness of various perioperative management strategies and to review and comment on a draft of the Advisory developed by the Task Force. Fourth, additional opinions were solicited from a random sample of active members of the ASA. Fifth, the Task Force held open forums at three national and international anesthesia meetings to solicit input on the key concepts of this Advisory. Sixth, all available information was used to build consensus within the Task Force on the Advisory.
The draft document was made available for review on the ASA Web site, and commentary was invited via e-mail announcement to all ASA members. All submitted comments were considered by the Task Force in preparing the final draft.
F. Availability and Strength of Evidence
Practice advisories are developed by a protocol similar to that of an ASA evidence-based practice guideline, including a systematic search and evaluation of the literature. However, practice advisories lack the support of a sufficient number of adequately controlled studies to permit aggregate analyses of data with rigorous statistical techniques such as meta-analysis. Nonetheless, literature-based evidence from case reports and other descriptive studies are considered during the development of the Advisory. This literature often permits the identification of recurring patterns of clinical practice.
As with a practice guideline, formal survey information is collected from consultants and members of the ASA. The following terms describe survey responses for any specified issue. Responses are solicited on a five-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree), with a score of 3 being equivocal. Survey responses are summarized based on median values as follows:
Strongly Agree: Median score of 5 (at least 50% of the responses are 5)
Agree: Median score of 4 (at least 50% of the responses are 4 or 4 and 5)
Equivocal: Median score of 3 (at least 50% of the responses are 3, or no other response category or combination of similar categories contain at least 50% of the responses)
Disagree: Median score of 2 (at least 50% of responses are 2 or 1 and 2)
Strongly Disagree: Median score of 1 (at least 50% of responses are 1)
Additional information is obtained from open forum presentations and other invited and public sources. The advisory statements contained in this document represent a distillation of the current spectrum of clinical opinion and literature-based findings (1).
Advisories
I. Preoperative Evaluation
A preoperative evaluation includes (1) obtaining a focused history (i.e. , medical records, laboratory reports, patient or patient-and-family interview), (2) conducting a physical examination, (3) identifying patients at risk for intraoperative awareness (e.g. , planned anesthetics, type of surgery), and (4) informing selected patients of the possibility of intraoperative awareness.
Descriptive studies and case reports suggest that certain patient characteristics may be associated with intraoperative awareness, including age, sex, ASA physical status, and drug resistance or tolerance.4,7–11 Descriptive studies and case reports suggest that certain procedures (e.g. , cesarean delivery, cardiac surgery, trauma surgery)4,8,12–29 as well as anesthetic techniques (e.g. , rapid-sequence induction, reduced anesthetic doses with or without the presence of paralysis)2,3,9,13,16,21,23,30–33 may be associated with an increased risk of intraoperative awareness. No studies were found that examined the clinical impact of informing the patient before surgery of the possibility of intraoperative awareness.
The consultants and ASA members agree that a preoperative evaluation may be helpful in identifying patients at risk for intraoperative awareness (2). In addition, they agree that a focused preoperative evaluation to identify patients at risk of intraoperative awareness should include review of a patient’s medical record, a thorough physical examination, and a patient or patient-and-family interview. They agree that patient characteristics that may place a patient at risk for intraoperative awareness include substance use or abuse, limited hemodynamic reserve, and ASA physical status of IV or V. The consultants strongly agree and the ASA members agree that a history of intraoperative awareness may place a patient at risk. The consultants disagree and the ASA members are equivocal regarding whether all patients should be informed of the possibility of intraoperative awareness. The consultants and ASA members agree that only patients considered to be at elevated risk of intraoperative awareness should be informed of the possibility of intraoperative awareness. Finally, the consultants and the ASA members disagree that informing the patient preoperatively of the risk of intraoperative awareness increases the actual risk of intraoperative awareness.
Advisory.
The Task Force believes that some components of the preoperative evaluation may be useful in identifying a patient at increased risk for awareness. An evaluation should include, if possible, a review of a patient’s medical records for previous occurrences of awareness or other potential risk factors, a patient interview to assess level of anxiety or previous experiences with anesthesia, and a physical examination. Potential risk factors to consider for patients undergoing general anesthesia include substance use or abuse (e.g. , opioids, benzodiazepines, cocaine), a history of awareness, a history of difficult intubation or anticipated difficult intubation, chronic pain patients using high doses of opioids, cardiac surgery, cesarean delivery, trauma and emergency surgery, reduced anesthetic doses in the presence of paralysis, planned use of muscle relaxants during the maintenance phase of general anesthesia, total intravenous anesthesia, the planned use of nitrous oxide-opioid anesthesia, ASA physical status of IV or V, and limited hemodynamic reserve. The consensus of the Task Force is that patients whom the individual clinician considers to be at substantially increased risk of intraoperative awareness should be informed of the possibility of intraoperative awareness when circumstances permit.
II. Preinduction Phase of Anesthesia
Issues regarding the preinduction phase of anesthesia related to the prevention of intraoperative awareness include checking the functioning of anesthesia delivery systems, and the prophylactic administration of benzodiazepines.
Although checking the functioning of anesthesia delivery systems is standard practice, some cases of intraoperative awareness have resulted from too-low concentrations of inspired volatile anesthetics or drug errors, including drug delivery errors.8,34–39 One double-blind randomized clinical trial evaluated the efficacy of the prophylactic administration of midazolam as an anesthetic adjuvant during ambulatory procedures under total intravenous anesthesia and reported a lower frequency of intraoperative awareness in the midazolam groups compared with the placebo group.40 Two randomized clinical trials examined anterograde amnesia by providing pictures as stimuli after administration of midazolam but before induction of general anesthesia. Although these studies reported reduced recall in patients administered midazolam, the presence of consciousness during general anesthesia and subsequent intraoperative awareness was not examined.41,42
The consultants and ASA members strongly agree that the functioning of anesthesia delivery systems (e.g. , vaporizers, infusion pumps, fresh gas flow, intravenous lines) should be checked to reduce the risk of intraoperative awareness. The consultants disagree and the ASA members are equivocal that a benzodiazepine or scopolamine should be used as a component of the anesthetic to reduce the risk of intraoperative awareness for all patients. The consultants agree that a benzodiazepine or scopolamine should be used for patients requiring smaller dosages of anesthetics, patients undergoing cardiac surgery, and patients undergoing trauma surgery. They are equivocal regarding patients undergoing cesarean delivery, emergency surgery, and total intravenous anesthesia. The ASA members agree that a benzodiazepine or scopolamine should be used for patients requiring smaller dosages of anesthetics and patients undergoing cardiac surgery, emergency surgery, trauma surgery, and total intravenous anesthesia. They are equivocal regarding patients undergoing cesarean delivery.
Advisory.
Because intraoperative awareness may be caused by equipment malfunction or misuse, the Task Force believes that there should be adherence to a checklist protocol for anesthesia machines and equipment to assure that the desired anesthetic drugs and doses will be delivered. These procedures should be extended to include verification of the proper functioning of intravenous access, infusion pumps, and their connections. The Task Force consensus is that the decision to administer a benzodiazepine prophylactically should be made on a case-by-case basis for selected patients (e.g. , patients requiring smaller dosages of anesthetics). The Task Force cautions that delayed emergence may accompany the use of benzodiazepines.
III. Intraoperative Monitoring
Intraoperative awareness cannot be measured during the intraoperative phase of general anesthesia, because the recall component of awareness can only be determined postoperatively by obtaining information directly from the patient. Therefore, the primary issue regarding intraoperative monitoring addressed by this Advisory is whether the use of clinical techniques, conventional monitoring systems, or brain function monitors reduces the occurrence of intraoperative awareness.
The majority of literature obtained during the search and review process did not directly address whether these techniques, systems, or monitors reduce the frequency of intraoperative awareness. However, many studies were found that report intraoperative measures or index values from monitoring activities. This literature, although not directly assessing the impact of an intervention on awareness, often reported patterns or values that occurred at identifiable times during the perioperative period with the intention of describing or predicting variations in the depth of anesthesia. Commonly reported findings from this literature are summarized below.
The literature for each intervention is presented in the following order: (1) randomized clinical trials, (2) nonrandomized comparative studies (e.g. , quasi-experimental, prospective cohort studies), (3) correlational studies (e.g. , correlations of index values with end-tidal concentrations of hypnotic drugs or with movement in response to noxious stimuli), (4) descriptive reports of monitored index values at particular times during a procedure, and (5) case reports of unusual or unintended benefits or harms occurring during a monitoring activity. Correlational studies often report a measure of association between two continuous variables (e.g. , the correlation between index values and anesthetic drug concentrations). Other correlational measures include a prediction probability (Pk) value that provides a measure of how well a monitor or technique can differentiate between two different clinical states (e.g. , response vs. no response to verbal command).43 A Pk value of 1.0 indicates perfect association between an index value and a clinical state, whereas a Pk value of 0.50 indicates a prediction probability equal to chance.
A. Clinical Techniques and Conventional Monitoring.
Among the clinical techniques used to assess intraoperative consciousness are checking for movement, response to commands, opened eyes, eyelash reflex, pupillary responses or diameters, perspiration, and tearing. Conventional monitoring systems include ASA standard monitoring3as well as the end-tidal anesthetic analyzer.
No clinical trials or other comparative studies were found that examine the effect of clinical techniques or conventional monitoring on the incidence of intraoperative awareness. Correlational studies reported Pk values ranging from 0.74 to 0.76 for the association between reflex or purposeful movement and indicators for depth of anesthesia.44 One study reported a significant association between response to command and memory when continuous infusions of propofol were used as the induction anesthetic.45 Pk values for mean arterial pressure (MAP) ranged from 0.68 to 0.94 for distinguishing a responsive state from an unresponsive state and from 0.81 to 0.89 for distinguishing an anesthetized state from emergence after anesthesia (i.e. , first response). Pk values for heart rate (HR) ranged from 0.50 to 0.82 for distinguishing a responsive state from an unresponsive state and from 0.54 to 0.67 for emergence.46–48 Wide ranges of mean MAP and HR values were reported during various intraoperative times. Studies reported ranges of mean MAP values as follows: before induction or baseline, 90–103 mmHg; at induction, 58.4–88 mmHg; during surgery, 78–102 mmHg; at emergence or end of surgery, 58.7–97 mmHg; and during postoperative recovery, 86–104 mmHg. Mean HR ranges were reported as follows: before induction or baseline, 61–82 beats/min; at induction, 55–67 beats/min; during surgery, 74–82 beats/min; at emergence or end of surgery, 59–92 beats/min; and during postoperative recovery, 82–89 beats/min.49–56 Awareness has been reported to occur in the absence of tachycardia or hypertension.8,23,24
The consultants and ASA members agree that clinical techniques (e.g. , checking for purposeful or reflex movement) are valuable and should be used to assess intraoperative consciousness. In addition, the consultants and ASA members agree that conventional monitoring systems (e.g. , electrocardiogram, blood pressure, HR, end-tidal anesthetic analyzer, capnography) are valuable and should be used to help assess intraoperative consciousness.
B. Brain Electrical Activity Monitoring.
Most of the devices designed to monitor brain electrical activity for the purpose of assessing anesthetic effect record electroencephalographic activity from electrodes placed on the forehead. Systems can be subdivided into those that process spontaneous electroencephalographic and electromyographic activity and those that acquire evoked responses to auditory stimuli (AEPs). After amplification and conversion of the analog electroencephalographic signal to the digital domain, various signal processing algorithms are applied to the frequency, amplitude, latency, and/or phase relationship data derived from the raw EEG or AEP to generate a single number, often referred to as an “index,” typically scaled between 0 and 100. This index represents the progression of clinical states of consciousness (“awake,”“sedated,”“light anesthesia,”“deep anesthesia”), with a value of 100 being associated with the awake state and values of 0 occurring with an isoelectric EEG (or absent middle latency AEP). These processing algorithms may either be published and in the public domain or proprietary. Detailed descriptions of the various approaches to electroencephalographic signal processing, including bispectral analysis, may be found elsewhere.57 Artifact recognition algorithms intended to avoid contaminated and therefore spurious “index” values are an important component of the software in most monitors.
Although electromyographic activity from scalp muscles can be considered an artifact from the viewpoint of pure electroencephalographic analysis, it may be an important source of clinically relevant information. Sudden appearance of frontal (forehead) electromyographic activity suggests somatic response to noxious stimulation resulting from inadequate analgesia and may give warning of impending arousal. For this reason, some monitors separately provide information on the level of electromyographic activity.
1. Spontaneous electroencephalographic activity monitors.
Bispectral Index. The Bispectral Index (BIS) is a proprietary algorithm (Aspect Medical Systems, Natick, MA) that converts a single channel of frontal electroencephalograph into an index of hypnotic level (BIS). BIS is available either as a separate device (BIS® monitor; Aspect Medical Systems) or incorporated, under license from Aspect Medical Systems, in “BIS modules” made by various anesthesia equipment manufacturers. To compute the BIS, several variables derived from the electroencephalographic time domain (burst-suppression analysis), frequency domain (power spectrum, bispectrum: interfrequency phase relationships) are combined into a single index of hypnotic level. BIS values are scaled from 0 to 100, with specific ranges (e.g. , 40–60) reported to reflect a low probability of consciousness under general anesthesia. The weight factors for the various components in the multivariate model that generates the BIS were empirically derived from a prospectively collected database of more than 1,500 anesthetics. The BIS® model accounts for the nonlinear stages of electroencephalographic activity by allowing different parameters to dominate the resulting BIS as the electroencephalographic changes its character with increasing plasma concentrations of various anesthetics, resulting in a linear decrease in BIS. As more data have become available and as methods and algorithms to suppress artifacts have been improved, revised iterations of the algorithm and optimized hardware have been released.
Several randomized controlled trials (RCTs) have compared outcomes with BIS-guided anesthetic administration versus standard clinical practice without BIS. In one RCT that enrolled 2,500 patients at high risk of intraoperative awareness, explicit recall occurred in 0.17% of patients when BIS monitors were used and in 0.91% of patients treated by routine clinical practice (P < 0.02).58 A small (n = 30), single-blinded RCT (i.e. , the anesthesiologists were blinded to the recorded BIS values) compared BIS monitoring with clinical signs during cardiac surgery and reported one episode of recall in the clinical signs group compared with no episodes in the BIS-monitored group (P > 0.50).59 In other RCTs, times to awakening, first response, or eye opening and consumption of anesthetic drugs were reduced with the use of BIS.8,60–68
One nonrandomized comparison of the use of BIS monitoring versus a cohort of historic controls (n = 12,771) found explicit recall occurring in 0.04% of the BIS-monitored patients versus 0.18% of the historic controls (P < 0.038).69 Another prospective nonrandomized cohort study (n = 19,575) designed to establish the incidence of awareness with recall during routine general anesthesia and to determine BIS values associated with intraoperative awareness events reported no statistically significant difference when BIS was used (0.18% of patients) compared with when BIS was not used (0.10% of patients).4 Other nonrandomized comparative studies reported higher index values on arrival in the postanesthesia care unit, shorter recovery times, and lower anesthetic use among patients monitored with BIS compared with patients not monitored with BIS.70,71 Numerous correlational studies reported Pk values for BIS ranging from 0.72 to 1.00 for awake versus loss of response after induction with propofol (with or without opioids) and from 0.79 to 0.97 for anesthetized versus first response.46–48,72–78 One study reported a Pk value of 0.86 for movement from electrical stimulation.44 Wide ranges of mean BIS values have been reported during various intraoperative times. Ranges of mean BIS values were as follows: before induction or baseline, 80–98; at or after induction, 37–70; during surgery, 20–58; at emergence or end of surgery, 42–96; and during postoperative recovery, 64–96.50,51,54-56,79-110 Several case reports indicate that intraoperative events unrelated to titration of anesthetic agents can produce rapid changes in BIS values (e.g. , cerebral ischemia or hypoperfusion, gas embolism, unrecognized hemorrhage, inadvertent blockage of anesthesia drug delivery).111–119 Other case reports suggest that routine intraoperative events (e.g. , administration of depolarizing muscle relaxants, activation of electromagnetic equipment or devices, patient warming or planned hypothermia) may interfere with BIS functioning.120–128 Two case reports were found that reported patients experiencing intraoperative awareness despite monitored values indicating an adequate depth of anesthesia.129,130 Finally, still other case reports suggested that certain patient conditions may affect BIS values.131–133
Entropy. Entropy (GE Healthcare Technologies, Waukesha, WI) describes the irregularity, complexity, or unpredictability characteristics of a signal. A single sine wave represents a completely predictable signal (entropy = 0), whereas noise from a random number generator represents entropy = 1. The algorithm for calculation of entropy in the electroencephalographic signal as incorporated in the Datex-Ohmeda S/5 entropy Module (Datex-Ohmeda, Inc., Madison, WI) is in the public domain, and detailed descriptions have recently been published.134
Entropy is independent of absolute scales such as the amplitude or the frequency of the signal. The commercially available Datex-Ohmeda module calculates entropy over time windows of variable duration and reports two separate entropy values. State entropy (SE) is an index ranging from 0 to 91 (awake), computed over the frequency range from 0.8 to 32 Hz, reflecting the cortical state of the patient. Response entropy (RE) is an index ranging from 0 to 100 (awake), computed over a frequency range from 0.8 to 47 Hz, containing the higher electromyographic-dominated frequencies, and will thus also respond to the increased electromyographic activity resulting from inadequate analgesia. No clinical trials or other comparative studies were found that examine the impact of entropy monitoring on the incidence of intraoperative awareness. One clinical trial reported reduced times to eye opening, response to command, and consumption of anesthetic drugs with the use of entropy monitoring.135
Correlational studies report the following Pk values for loss of consciousness: for RE, 0.83–0.97; for SE, 0.81–0.90.45,136–137 For anesthetized versus first response, the following Pk values are reported: for RE, 0.85; and for SE, 0.82.46 Ranges of mean RE and SE values were as follows: before induction or baseline, 98 (RE) and 89–91 (SE); during surgery, 34–52 (RE) and 50–63 (SE); and at emergence or end of surgery, 96 (RE) and 85 (SE).52,135,138,139
Narcotrend®. The Narcotrend® (MonitorTechnik, Bad Branstedt, Germany) is derived from a system developed for the visual classification of the electroencephalographic patterns associated with various stages of sleep. After artifact exclusion and Fourier transformation, the original electronic algorithm classified the raw (frontal) EEG according to the following system: A (awake), B (sedated), C (light anesthesia), D (general anesthesia), E (general anesthesia with deep hypnosis), F (general anesthesia with increasing burst suppression). The system included a series of subclassifications resulting in a total of 14 possible substages: A, B0–2, C0–2, D0–2, E0–1, and F0–1.140 In the most recent iteration of the Narcotrend® software (version 4.0), the alphabet-based scale has been “translated” into a dimensionless index, the Narcotrend® index, scaled from 0 (deeply anesthetized) to 100 (awake), with the stated intention of producing a scale quantitatively similar to the BIS index.
No clinical trials or other comparative studies were found that examine the impact of Narcotrend® monitoring on the incidence of intraoperative awareness. One RCT has compared the use of Narcotrend®-controlled versus clinically controlled anesthetic administration and found a shorter recovery time in the Narcotrend® group (i.e. , opened eyes) after termination of anesthesia.63 Pk values for Narcotrend® ranged from 0.93 to 0.99 for awake versus loss of response after induction with propofol combined with an opioid and from 0.94 to 0.99 for anesthetized versus first response.47,48 Reported mean Narcotrend® values are as follows: after induction (loss of response), 72–80; and at emergence or end of surgery (spontaneously opened eyes), 80.73
Patient state analyzer. The Patient State Index (PSI; Physiometrix, North Billerica, MA) is derived from a four-channel electroencephalograph. The derivation of the PSI is based on the observation that there are reversible spatial changes in power distribution of quantitative electroencephalograph at loss and return of consciousness. The PSI has a range of 0–100, with decreasing values indicating decreasing levels of consciousness or increasing levels of sedation, similar to BIS, entropy, and Narcotrend®. The PSI algorithm was constructed using stepwise, discriminant analysis based on multivariate combinations of quantitative electroencephalographic variables, derived after Fourier transformation of the raw EEG signal, and found to be sensitive to changes in the level of anesthesia.
No clinical trials or other comparative studies were found that examine the impact of PSI monitoring on the incidence of intraoperative awareness. One correlational study reported a Pk value of 0.70 for predicting response to command, with a sensitivity of 85.6% and specificity of 38.8%,77 and another study reported a significant correlation of the PSI with unconsciousness.141 Reported mean PSI values are as follows: before induction or baseline, 92; during surgery, 32; at emergence or end of surgery, 53; and during postoperative recovery, 81.141
SNAP index. The SNAPII (Everest Biomedical Instruments, Chesterfield, MO) calculates a “SNAP index” from a single channel of electroencephalograph. The index calculation is based on a spectral analysis of electroencephalographic activity in the 0 to 18 Hz and 80 to 420 Hz frequency ranges and a burst suppression algorithm. There are no published data on the actual algorithm used to calculate the SNAP index, which is based on a composite of both low-frequency (0–40 Hz) and high-frequency (80–420 Hz) components.
No clinical trials or other comparative studies were found that examine the impact of SNAP monitoring on the incidence of intraoperative awareness. One correlational study was found that reported a mean SNAP index of 71 to be predictive of a loss of consciousness in 95% of elective surgery patients.142
Cerebral State Monitor/Cerebral State Index. The Cerebral State Monitor (Danmeter A/S, Odense, Denmark) is a handheld device that analyzes a single channel EEG and presents a Cerebral State “Index” scaled from 0 to 100. In addition, it also provides electroencephalographic suppression percentage and a measure of electromyographic activity (75–85 Hz).
No published literature was found that examined the impact of using the Danmeter Cerebral State Monitor on the incidence of intraoperative awareness.
2. Evoked brain electrical activity monitors.
AEP Monitor/2 (Danmeter). Auditory evoked potentials are the electrical responses of the brainstem, the auditory radiation and the auditory cortex to auditory sound stimuli (clicks) delivered via headphones. The effects of anesthetics on AEP have been studied since the early 1980s.143–145 The brainstem response is relatively insensitive to anesthetics, whereas early cortical responses, known as the middle-latency AEPs (MLAEPs), change predictably with increasing concentrations of both volatile and intravenous anesthetics. The typical AEP response to increasing anesthetic concentrations is increased latency and decreased amplitude of the various waveform components. These signals are extremely small (< 1 μV), necessitating extraction from the spontaneous electroencephalograph using signal averaging techniques. Before recent innovations, signal averaging was relatively time consuming (several minutes per averaged waveform). More recent signal filtering advances have resulted in an instrument (A-Line®; Danmeter) that can record and rapidly update a single channel of AEPs from forehead electrodes. From a mathematical analysis of the AEP waveform, the device generates an “AEP-index” that provides a correlate of anesthetic concentration. The AEP index, or AAI, is scaled from 0 to 100. In contrast to many EEG indices, the AAI corresponding with low probability of consciousness is less than 25, rather than the higher numeric thresholds associated with the other monitors. The device is approved by the US Food and Drug Administration but is not currently marketed in North America.
Randomized controlled trials that compared MLAEP monitoring (e.g. , to titrate anesthetics) to standard clinical practice without MLAEPs reported reduced times to eye opening or orientation.63,64,146 A Pk value of 0.79 was reported for loss of eyelash reflex after induction with propofol and an opioid,74 and Pk values of 0.63 and 0.66 were reported for responsiveness after discontinuation of remifentanil or sevoflurane, respectively.147 One study reported a Pk value of 0.87 for movement,148 and another study reported a Pk value of 0.99 for awareness after laryngeal mask airway insertion.149 Descriptive studies reported ranges of mean values as follows: before induction or baseline, 73.5–85; at or after induction, 33.4–61; during surgery, 21.1–37.8; at emergence or end of surgery, 24.6–40; and during postoperative recovery, 89.7.74,80,144,150,151
C. Consultant and ASA Member Survey Findings.
Consultants who participated in this Advisory typically had either a particular knowledge or an expressed interest in intraoperative awareness and brain function monitors. The majority of these consultants disclosed receipt of funds from or a financial interest in a company developing or manufacturing brain function monitors. Consultants were not asked to disclose similar relationships with other companies that may be indirectly affected by the use of brain function monitors. ASA members were randomly selected from a list of active members of the society.
The consultants and ASA members disagree that a brain electrical activity monitor is valuable and should be used to reduce the risk of intraoperative awareness for all patients. The consultants and ASA members disagree that a brain electrical activity monitor is valuable and should be used to reduce the risk of intraoperative awareness for no patient. The consultants agree that a brain electrical activity monitor should be used for patients with conditions that may place them at risk and patients requiring smaller doses of general anesthetics, trauma surgery, cesarean delivery, and total intravenous anesthesia. They are equivocal regarding the use of brain electrical activity monitoring for cardiac surgery and emergency surgery. The ASA members agree with the use of such monitors for patients with conditions that may place them at risk, patients requiring smaller doses of general anesthetics, and patients undergoing cardiac surgery. They are equivocal regarding the use of these monitors for patients undergoing cesarean delivery, emergency surgery, trauma surgery, and total intravenous anesthesia.
The consultants and ASA members disagree that a brain electrical activity monitor is valuable and should be used to assess intraoperative depth of anesthesia for all patients. The consultants and ASA members disagree with the statement that “a brain electrical activity monitor is valuable and should be used to assess intraoperative depth of anesthesia for no patient.” The consultants agree that a brain electrical activity monitor should be used to assess intraoperative depth of anesthesia for selected patients. The ASA members agree with the use of brain electrical activity monitors for patients with conditions that may place them at risk and patients requiring smaller doses of general anesthetics. They are equivocal regarding the use of such monitors for patients undergoing cardiac surgery, cesarean delivery, emergency surgery, trauma surgery, and total intravenous anesthesia.
Advisory.
Intraoperative monitoring of depth of anesthesia, for the purpose of minimizing the occurrence of awareness, should rely on multiple modalities, including clinical techniques (e.g. , checking for clinical signs such as purposeful or reflex movement) and conventional monitoring systems (e.g. , electrocardiogram, blood pressure, HR, end-tidal anesthetic analyzer, capnography). The use of neuromuscular blocking drugs may mask purposeful or reflex movements and adds additional importance to the use of monitoring methods that assure the adequate delivery of anesthesia.
Brain function monitors are dedicated to the assessment of the effects of anesthetics on the brain and provide information that correlates with some depth of anesthesia indicators, such as plasma concentrations of certain anesthetics (e.g. , propofol). In general, the indices generated by these monitors vary in parallel with other established correlates of depth of anesthesia, although the values generated by individual devices in any given anesthetic state differ among the various monitoring technologies. In addition, the values generated by individual devices in the face of a given depth of anesthesia achieved by different combinations of anesthetic drugs (e.g. , with or without opioids) also differ. In other words, a specific numerical value may not correlate with a specific depth of anesthesia. Furthermore, the measured values do not have uniform sensitivity across different anesthetic drugs or types of patients. As with other monitors, common occurrences in the operating room may introduce artifacts into the values derived by these monitors (e.g. , electrocautery, lasers, warming devices).
The general clinical applicability of these monitors in the prevention of intraoperative awareness has not been established. Although a single randomized clinical trial reported a decrease in the frequency of awareness in high-risk patients, there is insufficient evidence to justify a standard, guideline, or absolute requirement that these devices be used to reduce the occurrence of intraoperative awareness in high-risk patients undergoing general anesthesia. In addition, there is insufficient evidence to justify a standard, guideline, or absolute requirement that these devices be used to reduce the occurrence of intraoperative awareness for any other group of patients undergoing general anesthesia.
It is the consensus of the Task Force that brain function monitoring is not routinely indicated for patients undergoing general anesthesia, either to reduce the frequency of intraoperative awareness or to monitor depth of anesthesia. This consensus is based, in part, on the state of the literature and survey responses from the consultants and ASA membership, who generally disagree with the following statements: “Brain function monitors are valuable and should be used to reduce the risk of intraoperative awareness for all patients under general anesthesia,” and “brain function monitors are valuable and should be used when possible to assess intraoperative depth of anesthesia for all patients under general anesthesia” (2).
It is the consensus of the Task Force that the decision to use a brain function monitor should be made on a case-by-case basis by the individual practitioner for selected patients (e.g. , light anesthesia). This consensus is based, in part, on the state of the literature and survey response patterns from consultants and ASA members regarding specific risk factors (2). The Task Force cautions that maintaining low brain function monitor values in an attempt to prevent intraoperative awareness may conflict with other important anesthesia goals (e.g. , preservation of vital organ functions, minimizing the risks of aggravating existing comorbidities152). It is the opinion of the Task Force that brain function monitors currently have the status of the many other monitoring modalities that are currently used in selected situations at the discretion of individual clinicians.
IV. Intraoperative and Postoperative Interventions
Intraoperative and postoperative interventions include (1) the intraoperative administration of benzodiazepines to patients who may have become conscious, (2) providing a postoperative structured interview to patients to define the nature of the episode after an episode of intraoperative awareness has been reported, (3) providing a postoperative questionnaire to patients to define the nature of the episode, and (4) offering postoperative counseling or psychological support.
No studies were found that evaluated the efficacy of the intraoperative administration of benzodiazepines to patients who have unexpectedly become conscious in reducing the occurrence of awareness. Two randomized clinical trials examined retrograde amnesia by providing pictures as stimuli to awake patients before administration of midazolam and induction of general anesthesia. The studies reported no evidence of retrograde amnesia.41,42 However, these studies did not examine the effect of administering a benzodiazepine to patients after the apparent occurrence of consciousness during general anesthesia.
Although several studies have applied structured interviews and questionnaires to obtain additional information about reported incidences of intraoperative awareness,4,11,26,28,153–157 no studies were found that demonstrated improvements in patient well-being or psychological state after such interactions. No studies were found that followed up on the efficacy of counseling or psychological support provided to patients who experienced a documented incidence of intraoperative awareness.
The consultants are equivocal and ASA members agree that benzodiazepines or scopolamine should be administered intraoperatively to prevent awareness after a patient has unexpectedly become conscious. The consultants strongly agree and the ASA members agree that once an episode of intraoperative awareness has been reported, a structured interview should be conducted to define the nature of the episode. Both the consultants and ASA members are equivocal regarding whether a questionnaire should be given to define the nature of the episode. The consultants strongly agree and the ASA members agree that in documented cases of intraoperative awareness, patients should be offered counseling or psychological support. Finally, the consultants strongly agree and the ASA members agree that in documented cases of intraoperative awareness, an occurrence report regarding the event should be completed for the purpose of quality management.
Advisory.
The Task Force consensus is that the decision to administer a benzodiazepine intraoperatively after a patient unexpectedly becomes conscious should be made on a case-by-case basis. This consensus is based, in part, on the state of the literature and on responses from the consultants and ASA members regarding the following statement: “Benzodiazepines or scopolamine should be administered intraoperatively to prevent awareness after a patient has unexpectedly become conscious.” However, the Task Force believes that evidence from the literature is not sufficient to provide guidance regarding this issue. Finally, the Task Force cautions that the use of scopolamine may result in unintended side effects (e.g. , emergence delirium).
Practitioners should speak with patients who report recall of intraoperative events to obtain details of the event and to discuss possible reasons for its occurrence.4A questionnaire or structured interview may be used to obtain a detailed account of the patient’s experience. Once an episode of intraoperative awareness has been reported, an occurrence report regarding the event should be completed for the purpose of quality management. Finally, the patient should be offered counseling or psychological support.
References#
- Myles PS, Williams D, Hendrata M, Anderson H, Weeks A: Patient satisfaction after anaesthesia and surgery: Results of a prospective survey of 10,811 patients. Br J Anaesth 2000; 84:6–10Myles, PS Williams, D Hendrata, M Anderson, H Weeks, A
- Nordstrom O, Engstrom AM, Persson S, Sandin R: Incidence of awareness in total i.v. anaesthesia based on propofol, alfentanil and neuromuscular blockade. Acta Anaesthesiol Scand 1997; 41:978–84Nordstrom, O Engstrom, AM Persson, S Sandin, R
- Sandin RH, Enlund G, Samuelsson P, Lennmarken C: Awareness during anaesthesia: A prospective case study. Lancet 2000; 355:707–11Sandin, RH Enlund, G Samuelsson, P Lennmarken, C
- Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB: The incidence of awareness during anesthesia: A multicenter United States study. Anesth Analg 2004; 99:833–9Sebel, PS Bowdle, TA Ghoneim, MM Rampil, IJ Padilla, RE Gan, TJ Domino, KB
- Lennmarken C, Bildfors K, Enlund G, Samuelsson P, Sandin R: Victims of awareness. Acta Anaesthesiol Scand 2002; 46:229–31Lennmarken, C Bildfors, K Enlund, G Samuelsson, P Sandin, R
- Schacter DL: Implicit expressions of memory in organic amnesia: Learning of new facts and associations. Hum Neurobiol 1987; 6:107–18Schacter, DL
- Brundidge PK, Leavell ME, Tempelhoff R: EEG-controlled “overdosage” of anesthetics in a patient with a history of intra-anesthetic awareness. J Clin Anesth 1994; 6:496–9Brundidge, PK Leavell, ME Tempelhoff, R
- Domino KB, Posner KL, Caplan RA, Cheney FW: Awareness during anesthesia: A closed claims analysis. Anesthesiology 1999; 90:1053–61Domino, KB Posner, KL Caplan, RA Cheney, FW
- Gan TJ, Glass PS, Sigl J, Sebel P, Payne F, Rosow C, Embree P: Women emerge from general anesthesia with propofol/alfentanil/nitrous oxide faster than men. Anesthesiology 1999; 90:1283–7Gan, TJ Glass, PS Sigl, J Sebel, P Payne, F Rosow, C Embree, P
- Lopez U, Iselin-Chaves I, Habre W, Van der Linden M: Incidence of awareness during general anaesthesia in children. Br J Anaesth 2004; 93:490P–1PLopez, U Iselin-Chaves, I Habre, W Van der Linden, M
- Lopez-Candel E, Canovas E, Lopez-Candel J, Garcia R, Soler J, Fernandez S, Hernandez JP, Vargas J: Awareness: Report of a case in pediatric surgery. Cirugia Pediatr 2000; 13:81–3Lopez-Candel, E Canovas, E Lopez-Candel, J Garcia, R Soler, J Fernandez, S Hernandez, JP Vargas, J
- Adams DC, Hilton HJ, Madigan JD, Szerlip NJ, Cooper LA, Emerson RG, Smith CR, Rose EA, Oz MC: Evidence for unconscious memory processing during elective cardiac surgery. Circulation 1998; 98:II289–92Adams, DC Hilton, HJ Madigan, JD Szerlip, NJ Cooper, LA Emerson, RG Smith, CR Rose, EA Oz, MC
- Baraka A, Siddik S, Assaf B: Supplementation of general anaesthesia with tramadol or fentanyl in parturients undergoing elective caesarean section. Can J Anaesth 1998; 45:631–4Baraka, A Siddik, S Assaf, B
- Bogetz MS, Katz JA: Recall of surgery for major trauma. Anesthesiology 1984; 61:6–9Bogetz, MS Katz, JA
- Bogod DG, Orton JK, Yau HM, Oh TE: Detecting awareness during general anaesthetic caesarean section: An evaluation of two methods. Anaesthesia 1990; 45:279–84Bogod, DG Orton, JK Yau, HM Oh, TE
- Brahams D: Caesarean section: Pain and awareness without negligence. Anaesthesia 1990; 45:161–2Brahams, D
- Gilron I, Solomon P, Plourde G: Unintentional intraoperative awareness during sufentanil anaesthesia for cardiac surgery. Can J Anaesth 1996; 43:295–8Gilron, I Solomon, P Plourde, G
- Goldmann L, Shah MV, Hebden MW: Memory of cardiac anaesthesia: Psychological sequelae in cardiac patients of intra-operative suggestion and operating room conversation. Anaesthesia 1987; 42:596–603Goldmann, L Shah, MV Hebden, MW
- Jeon SY, Lim HJ, Cho H, Lee BW: Awareness detection during a cesarean section under general anesthesia using bispectral index monitoring. Korean J Anesth 2000; 39:632–7Jeon, SY Lim, HJ Cho, H Lee, BW
- Lubke GH, Kerssens C, Gershon RY, Sebel PS: Memory formation during general anesthesia for emergency cesarean sections. Anesthesiology 2000; 92:1029–34Lubke, GH Kerssens, C Gershon, RY Sebel, PS
- Lyons G, Macdonald R: Awareness during caesarean section. Anaesthesia 1991; 46:62–4Lyons, G Macdonald, R
- Mark JB, Greenberg LM: Intraoperative awareness and hypertensive crisis during high-dose fentanyl-diazepam-oxygen anesthesia. Anesth Analg 1983; 62:698–700Mark, JB Greenberg, LM
- Moerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, D’Hont L, Rolly G: Awareness during anaesthesia for implantable cardioverter defibrillator implantation: Recall of defibrillation shocks. Anaesthesia 1995; 50:733–5Moerman, A Herregods, L Foubert, L Poelaert, J Jordaens, L D’Hont, L Rolly, G
- Moerman N, Bonke B, Oosting J: Awareness and recall during general anesthesia: Facts and feelings. Anesthesiology 1993; 79:454–64Moerman, N Bonke, B Oosting, J
- Phillips AA, McLean RF, Devitt JH, Harrington EM: Recall of intraoperative events after general anaesthesia and cardiopulmonary bypass. Can J Anaesth 1993; 40:922–6Phillips, AA McLean, RF Devitt, JH Harrington, EM
- Ranta SO, Herranen P, Hynynen M: Patients’ conscious recollections from cardiac anesthesia. J Cardiothorac Vasc Anesth 2002; 16:426–30Ranta, SO Herranen, P Hynynen, M
- Ranta SO, Jussila J, Hynyen M: Recall of awareness during cardiac anaesthesia: Influence of feedback information to the anaesthesiologist. Acta Anaesth Scand 1996; 40:554–60Ranta, SO Jussila, J Hynyen, M
- Russell IF, Wang M: Absence of memory for intraoperative information during surgery under adequate general anaesthesia. Br J Anaesth 1997; 78:3–9Russell, IF Wang, M
- Schultetus RR, Hill CR, Dharamraj CM, Banner TE, Berman LS: Wakefulness during cesarean section after anesthetic induction with ketamine, thiopental, or ketamine and thiopental combined. Anesth Analg 1986; 65:723–8Schultetus, RR Hill, CR Dharamraj, CM Banner, TE Berman, LS
- Dowd NP, Cheng DC, Karski JM, Wong DT, Munro JA, Sandler AN: Intraoperative awareness in fast-track cardiac anesthesia. Anesthesiology 1998; 89:1068–73Dowd, NP Cheng, DC Karski, JM Wong, DT Munro, JA Sandler, AN
- Ranta SO, Laurila R, Saario J, Ali-Melkkila T, Hynynen M: Awareness with recall during general anesthesia: Incidence and risk factors. Anesth Analg 1998; 86:1084–1089Ranta, SO Laurila, R Saario, J Ali-Melkkila, T Hynynen, M
- Rowan KJ: Awareness under TIVA: A doctor’s personal experience. Anesth Intensive Care 2002; 30:505–6Rowan, KJ
- Sandin RH, Norstrom O: Awareness during total i.v. anaesthesia. Br J Anaesth 1993; 71:782–7Sandin, RH Norstrom, O
- Bergman IJ, Kluger MT, Short TG: Awareness during general anaesthesia: A review of 81 cases from the Anaesthetic Incident Monitoring Study. Anaesthesia 2002; 57:549–56Bergman, IJ Kluger, MT Short, TG
- Caplan RA, Vistica MF, Posner KL, Cheney FW: Adverse anesthetic outcomes arising from gas delivery equipment. Anesthesiology 1997; 87:741–8Caplan, RA Vistica, MF Posner, KL Cheney, FW
- Lamberty JM, Lerman J: Intraoperative failure of a Fluotec Mark II vapourizer. Can Anaesth Soc J 1984; 31:687–9Lamberty, JM Lerman, J
- Masuda A, Arai Y, Hirota K, Shibuya N, Ito Y: Misuse of infusion pump during propofol anaesthesia. Can J Anaesth 1998; 145:187–8Masuda, A Arai, Y Hirota, K Shibuya, N Ito, Y
- Slinger PD, Scott WA, Kliffer AP: Intraoperative awareness due to malfunction of a Siemens 900B ventilator. Can J Anaesth 1990; 37:258–61Slinger, PD Scott, WA Kliffer, AP
- Tong D, Chung F: Recall after total intravenous anaesthesia due to an equipment misuse. Can J Anaesth 1997; 44:73–7Tong, D Chung, F
- Miller DR, Blew PG, Martineau RJ, Hull KA: Midazolam and awareness with recall during total intravenous anaesthesia. Can J Anaesth 1996; 43:946–53Miller, DR Blew, PG Martineau, RJ Hull, KA
- Bulach R, Myles PS, Russnak M: Double-blind randomized controlled trial to determine extent of amnesia with midazolam given immediately before general anesthesia. Br J Anaesth 2005; 94:300–5Bulach, R Myles, PS Russnak, M
- Twersky RS, Hartung J, Berger BJ, McClain J, Beaton C: Midazolam enhances anterograde but not retrograde amnesia in pediatric patients. Anesthesiology 1993; 78:51–5Twersky, RS Hartung, J Berger, BJ McClain, J Beaton, C
- Smith WD, Dutton RC, Smith NT: Measuring the performance of anesthetic depth indicators. Anesthesiology 1996; 84:38–51Smith, WD Dutton, RC Smith, NT
- Leslie K, Sessler DI, Smith WD, Larson MD, Ozaki M, Blanchard D, Crankshaw DP: Prediction of movement during propofol/nitrous oxide anesthesia: Performance of concentration, electroencephalographic, pupillary, and hemodynamic indicators. Anesthesiology 1996; 84:52–63Leslie, K Sessler, DI Smith, WD Larson, MD Ozaki, M Blanchard, D Crankshaw, DP
- Dutton RC, Smith WD, Smith NT: Wakeful response to command indicates memory potential during emergence from general anesthesia. J Clin Monit 1995; 11:35–40Dutton, RC Smith, WD Smith, NT
- Schmidt G, Bischoff P, Standl T, Hellstern A, Teuber O, Schulte am Esch J: Comparative evaluation of the Datex-Ohmeda S/5 entropy module and the Bispectral Index monitor during propofol–remifentanil anesthesia. Anesthesiology 2004; 101:1283–90Schmidt, G Bischoff, P Standl, T Hellstern, A Teuber, O Schulte am Esch, J
- Schmidt GN, Bischoff P, Standl T, Jensen K, Voigt M, Schulte Am Esch J: Narcotrend and Bispectral Index monitor are superior to classic electroencephalographic parameters for the assessment of anesthetic states during propofol–remifentanil anesthesia. Anesthesiology 2003; 99:1072–7Schmidt, GN Bischoff, P Standl, T Jensen, K Voigt, M Schulte Am Esch, J
- Schmidt GN, Bischoff P, Standl T, Lankenau G, Hilbert M, Schulte am Esch J: Comparative evaluation of Narcotrend, bispectral index, and classical electroencephalographic variables during induction, maintenance, and emergence of a propofol/remifentanil anesthesia. Anesth Analg 2004; 98:1346–53Schmidt, GN Bischoff, P Standl, T Lankenau, G Hilbert, M Schulte am Esch, J
- Atallah MM, el-Mohayman HA, el-Metwally RE: Ketamine-midazolam total intravenous anaesthesia for prolonged abdominal surgery. Eur J Anaesthesiol 2001; 18:29–35Atallah, MM el-Mohayman, HA el-Metwally, RE
- Coste C, Guignard B, Menigaux C, Chauvin M: Nitrous oxide prevents movement during orotracheal intubation without affecting BIS value. Anesth Analg 2000; 91:130–5Coste, C Guignard, B Menigaux, C Chauvin, M
- Hackner C, Detsch O, Schneider G, Jelen-Esselborn S, Kochs E: Early recovery after remifentanil-pronounced compared with propofol-pronounced total intravenous anaesthesia for short painful procedures. Br J Anaesth 2003; 91:580–2Hackner, C Detsch, O Schneider, G Jelen-Esselborn, S Kochs, E
- Iannuzzi M, Iannuzzi E, Rossi F, Berrino L, Chiefari M: Relationship between bispectral index, electroencephalographic state entropy and effect-site EC50 for propofol at different clinical endpoints. Br J Anaesth 2005; 94:613–6Iannuzzi, M Iannuzzi, E Rossi, F Berrino, L Chiefari, M
- Lehmann A, Zeitler C, Thaler E, Isgro F, Boldt J: Comparison of two different anesthesia regimens in patients undergoing aortocoronary bypass grafting surgery: Sufentanil-midazolam versus remifentanil-propofol. J Cardiothorac Vasc Anesth 2000; 14:416–20Lehmann, A Zeitler, C Thaler, E Isgro, F Boldt, J
- McCann ME, Brustowicz RM, Bacsik J, Sullivan L, Auble SG, Laussen PC: The bispectral index and explicit recall during the intraoperative wake-up test for scoliosis surgery. Anesth Analg 2002; 94:1474–8McCann, ME Brustowicz, RM Bacsik, J Sullivan, L Auble, SG Laussen, PC
- McDonald T, Hoffman WE, Berkowitz R, Cunningham F, Cooke B: Heart rate variability and plasma catecholamines in patients during opioid detoxification. J Neurosurg Anesthesiol 1999; 11:195–9McDonald, T Hoffman, WE Berkowitz, R Cunningham, F Cooke, B
- Ting CK, Hu JS, Teng YH, Chang YY, Tsou MY, Tsai SK: Desflurane accelerates patient response during the wake-up test for scoliosis surgery. Can J Anesth 2004; 51:393–397Ting, CK Hu, JS Teng, YH Chang, YY Tsou, MY Tsai, SK
- Rampil IJ: A primer for EEG signal processing in anesthesia. Anesthesiology 1998; 89:980–1002Rampil, IJ
- Myles PS, Leslie K, McNeil J, Forbes A, Chan MTV: Bispectral index monitoring to prevent awareness during anaesthesia: The B-aware randomised controlled trial. Lancet 2004; 363:1757–63Myles, PS Leslie, K McNeil, J Forbes, A Chan, MTV
- Puri GD, Murthy SS: Bispectral index monitoring in patients undergoing cardiac surgery under cardiopulmonary bypass. Eur J Anaesth 2003; 20:451–6Puri, GD Murthy, SS
- Bannister CF, Brosius KK, Sigl JC, Meyer BJ, Sebel PS: The effect of bispectral index monitoring on anesthetic use and recovery in children anesthetized with sevoflurane in nitrous oxide. Anesth Analg 2001; 92:877–1Bannister, CF Brosius, KK Sigl, JC Meyer, BJ Sebel, PS
- Basar H, Ozcan S, Buyukkocak U, Akpinar S, Apan A: Effect of bispectral index monitoring on sevoflurane consumption. Eur JAnaesth 2003; 20:396–400Basar, H Ozcan, S Buyukkocak, U Akpinar, S Apan, A
- Gan TJ, Glass PS, Windsor A, Payne F, Rosow C, Sebel P, Manberg P: Bispectral Index monitoring allows faster emergence and improved recovery from propofol, alfentanil, and nitrous oxide anesthesia. Anesthesiology 1997; 87:808–15Gan, TJ Glass, PS Windsor, A Payne, F Rosow, C Sebel, P Manberg, P
- Kreuer S, Biedler A, Larsen R, Altmann S, Wilhelm W: Narcotrend monitoring allows faster emergence and a reduction of drug consumption in propofol–remifentanil anesthesia. Anesthesiology 2003; 99:34–41Kreuer, S Biedler, A Larsen, R Altmann, S Wilhelm, W
- Recart A, Gasanova I, White PF, Thomas T, Ogunnaike B, Hamza M, Wang A: The effect of cerebral monitoring on recovery after general anesthesia: A comparison of the auditory evoked potential and bispectral index devices with standard clinical practice. Anesth Analg 2003; 97:1667–74Recart, A Gasanova, I White, PF Thomas, T Ogunnaike, B Hamza, M Wang, A
- Song D, Joshi GP, White PF: Titration of volatile anesthetics using Bispectral Index facilitates recovery after ambulatory anesthesia. Anesthesiology 1997; 87:842–8Song, D Joshi, GP White, PF
- White PF, Ma H, Tang J, Wender RH, Sloninsky A, Kariger R: Does the use of electroencephalographic Bispectral Index or auditory evoked potential index monitoring facilitate recovery after desflurane anesthesia in the ambulatory setting? Anesthesiology 2004; 100:811–7White, PF Ma, H Tang, J Wender, RH Sloninsky, A Kariger, R
- Wong J, Song D, Blanshard H, Grady D, Chung F: Titration of isoflurane using BIS index improves early recovery of elderly patients undergoing orthopedic surgeries. Can J Anaesth 2002; 49:13–8Wong, J Song, D Blanshard, H Grady, D Chung, F
- Yli-Hankala A, Vakkuri A, Annila P, Korttila K: EEG bispectral index monitoring in sevoflurane or propofol anaesthesia: Analysis of direct costs and immediate recovery. Acta Anaesthesiol Scand 1999; 43:545–9Yli-Hankala, A Vakkuri, A Annila, P Korttila, K
- Ekman A, Lindholm ML, Lennmarken C, Sandin R: Reduction in the incidence of awareness using BIS monitoring. Acta Anaesth Scand 2004; 48:20–6Ekman, A Lindholm, ML Lennmarken, C Sandin, R
- Burrow B, McKenzie B, Case C: Do anaesthetized patients recover better after bispectral index monitoring? Anaesth Intensive Care 2001; 29:239–45Burrow, B McKenzie, B Case, C
- Guignard B, Coste C, Menigaux C, Chauvin M: Reduced isoflurane consumption with bispectral index monitoring. Acta Anaesthesiol Scand 2001; 45:308–4Guignard, B Coste, C Menigaux, C Chauvin, M
- Glass PS, Bloom M, Kearse L, Rosow C, Sebel P, Manberg P: Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy individuals. Anesthesiology 1997; 86:836–7Glass, PS Bloom, M Kearse, L Rosow, C Sebel, P Manberg, P
- Kreuer S, Bruhn J, Larsen R, Bialas P, Wilhelm W: Comparability of Narcotrend index and bispectral index during propofol anaesthesia. Br J Anaesth 2004; 93:235–40Kreuer, S Bruhn, J Larsen, R Bialas, P Wilhelm, W
- Kreuer S, Bruhn J, Larsen R, Hoepstein M, Wilhelm W: Comparison of Alaris AEP index and bispectral index during propofol-remifentanil anaesthesia. Br J Anaesth 2003; 91:336–40Kreuer, S Bruhn, J Larsen, R Hoepstein, M Wilhelm, W
- Lysakowski C, Dumont L, Pellegrini M, Clergue F, Tassonyi E: Effects of fentanyl, alfentanil, remifentanil and sufentanil on loss of consciousness and bispectral index during propofol induction of anaesthesia. Br J Anaesth 2001; 86:523–7Lysakowski, C Dumont, L Pellegrini, M Clergue, F Tassonyi, E
- Schmidt GN, Bischoff P, Standl T, Issleib M, Voigt M, Schulte Am Esch J: ARX-derived auditory evoked potential index and bispectral index during the induction of anesthesia with propofol and remifentanil. Anesth Analg 2003; 97:139–44Schmidt, GN Bischoff, P Standl, T Issleib, M Voigt, M Schulte Am Esch, J
- Schneider G, Gelb AW, Schmeller B, Tschakert R, Kochs E: Detection of awareness in surgical patients with EEG-based indices: Bispectral index and patient state index. Br J Anaesth 2003; 91:329–35Schneider, G Gelb, AW Schmeller, B Tschakert, R Kochs, E
- Schraag S, Bothner U, Gajraj R, Kenny GN, Georgieff M: The performance of electroencephalogram bispectral index and auditory evoked potential index to predict loss of consciousness during propofol infusion. Anesth Analg 1999; 89:1311–5Schraag, S Bothner, U Gajraj, R Kenny, GN Georgieff, M
- Absalom AR, Sutcliffe N, Kenny GN: Closed-loop control of anesthesia using Bispectral Index: Performance assessment in patients undergoing major orthopedic surgery under combined general and regional anesthesia. Anesthesiology 2002; 96:67–73Absalom, AR Sutcliffe, N Kenny, GN
- Anderson RE, Barr G, Assareh H, Jakobsson J: The AAI index, the BIS index and end-tidal concentration during wash in and wash out of sevoflurane. Anaesthesia 2003; 58:531–5Anderson, RE Barr, G Assareh, H Jakobsson, J
- Barvais L, Engelman E, Eba JM, Coussaert E, Cantraine F, Kenny GN: Effect site concentrations of remifentanil and pupil response to noxious stimulation. Br J Anaesth 2003; 91:347–52Barvais, L Engelman, E Eba, JM Coussaert, E Cantraine, F Kenny, GN
- Billard V, Gambus PL, Chamoun N, Stanski DR, Shafer SL: A comparison of spectral edge, delta power, and bispectral index as EEG measures of alfentanil, propofol, and midazolam drug effect. Clin Pharmacol Ther 1997; 61:45–58Billard, V Gambus, PL Chamoun, N Stanski, DR Shafer, SL
- Brosius KK, Bannister CF: Oral midazolam premedication in preadolescents and adolescents. Anesth Analg 2002; 94:31–6Brosius, KK Bannister, CF
- Chawathe MS, Francis V, Hall JE, Mecklenburth JS, Aguilera IM: Interpretation of BIS values in children using aspect 2000 monitor during i.v. induction. Br J Anaesth 2004; 92:301P–2PChawathe, MS Francis, V Hall, JE Mecklenburth, JS Aguilera, IM
- Choudhry DK, Brenn BR: Bispectral index monitoring: A comparison between normal children and children with quadriplegic cerebral palsy. Anesth Analg 2002; 95:1582–5Choudhry, DK Brenn, BR
- Denman WT, Swanson EL, Rosow D, Ezbicki K, Connors PD, Rosow CE: Pediatric evaluation of the bispectral index (BIS) monitor and correlation of BIS with end-tidal sevoflurane concentration in infants and children. Anesth Analg 2000; 90:872–7Denman, WT Swanson, EL Rosow, D Ezbicki, K Connors, PD Rosow, CE
- El-Kerdawy HM, Zalingen EE, Bovill JG: The influence of the alpha2-adrenoceptor agonist, clonidine, on the, EEG, and on the MAC of isoflurane. Eur J Anaesth 2000; 17:105–10El-Kerdawy, HM Zalingen, EE Bovill, JG
- Flaishon R, Windsor A, Sigl J, Sebel PS: Recovery of consciousness after thiopental or propofol: Bispectral Index and isolated forearm technique. Anesthesiology 1997; 86:613–9Flaishon, R Windsor, A Sigl, J Sebel, PS
- Friedberg BL: The effect of a dissociative dose of ketamine on the bispectral index (BIS) during propofol hypnosis. J Clin Anesth 1999; 11:4–7Friedberg, BL
- Gajraj RJ, Doi M, Mantzaridis H, Kenny GN: Comparison of bispectral EEG analysis and auditory evoked potentials for monitoring depth of anaesthesia during propofol anaesthesia. Br J Anaesth 1999; 82:672–8Gajraj, RJ Doi, M Mantzaridis, H Kenny, GN
- Gale T, Leslie K, Kluger M: Propofol anaesthesia via target controlled infusion or manually controlled infusion: Effects on the bispectral index as a measure of anaesthetic depth. Anaesth Intensive Care 2001; 29:579–84Gale, T Leslie, K Kluger, M
- Goto T, Nakata Y, Saito H, Ishiguro Y, Niimi Y, Suwa K, Morita S: Bispectral analysis of the electroencephalogram does not predict responsiveness to verbal command in patients emerging from xenon anaesthesia. Br J Anaesth 2000; 85:359–63Goto, T Nakata, Y Saito, H Ishiguro, Y Niimi, Y Suwa, K Morita, S
- Greif R, Greenwald S, Schweitzer E, Laciny S, Rajek A, Caldwell JE, Sessler DI: Muscle relaxation does not alter hypnotic level during propofol anesthesia. Anesth Analg 2002; 94:604–8Greif, R Greenwald, S Schweitzer, E Laciny, S Rajek, A Caldwell, JE Sessler, DI
- Gunawardane PO, Murphy PA, Sleigh JW: Bispectral index monitoring during electroconvulsive therapy under propofol anaesthesia. Br J Anaesth 2002; 88:184–7Gunawardane, PO Murphy, PA Sleigh, JW
- Jellish WS, Leonetti JP, Avramov A, Fluder E, Murdoch J: Remifentanil-based anesthesia versus a propofol technique for otologic surgical procedures. Otolaryngol Head Neck Surg 2000; 122:222–7Jellish, WS Leonetti, JP Avramov, A Fluder, E Murdoch, J
- Kim DW, Kil HY, White PF: Relationship between clinical endpoints for induction of anesthesia and bispectral index and effect-site concentration values. J Clin Anesth 2002; 14:241–5Kim, DW Kil, HY White, PF
- Kuizenga K, Wierda JM, Kalkman CJ: Biphasic EEG changes in relation to loss of consciousness during induction with thiopental, propofol, etomidate, midazolam or sevoflurane. Br J Anaesth 2001; 86:354–60Kuizenga, K Wierda, JM Kalkman, CJ
- McDonald TB, Berkowitz RA, Hoffman WE: Median EEG frequency is more sensitive to increases in sympathetic activity than bispectral index. J Neurosurg Anesth 1999; 11:255–9McDonald, TB Berkowitz, RA Hoffman, WE
- Menigaux C, Guignard B, Adam F, Sessler DI, Joly V, Chauvin M: Esmolol prevents movement and attenuates the BIS response to orotracheal intubation. Br J Anaesth 2002; 89:857–62Menigaux, C Guignard, B Adam, F Sessler, DI Joly, V Chauvin, M
- Mi W, Sakai T, Kudo T, Kudo M, Matsuki A: The interaction between fentanyl and propofol during emergence from anesthesia: Monitoring with the EEG-Bispectral index. J Clin Anesth 2003; 15:103–7Mi, W Sakai, T Kudo, T Kudo, M Matsuki, A
- Mi WD, Sakai T, Singh H, Kudo T, Kudo M, Matsuki A: Hypnotic endpoints vs. the bispectral index, 95% spectral edge frequency and median frequency during propofol infusion with or without fentanyl. Eur J Anaesth 1999; 16:47–52Mi, WD Sakai, T Singh, H Kudo, T Kudo, M Matsuki, A
- Mi WD, Sakai T, Takahashi S, Matsuki A: Haemodynamic and electroencephalograph responses to intubation during induction with propofol or propofol/fentanyl. Can J Anaesth 1998; 45:19–22Mi, WD Sakai, T Takahashi, S Matsuki, A
- Sakai T, Singh H, Mi WD, Kudo T, Matsuki A: The effect of ketamine on clinical endpoints of hypnosis and EEG variables during propofol infusion. Acta Anaesthesiol Scand 1999; 43:212–6Sakai, T Singh, H Mi, WD Kudo, T Matsuki, A
- Shao X, Li H, White PF, Klein KW, Kulstad C, Owens A: Bisulfite-containing propofol: Is it a cost-effective alternative to Diprivan for induction of anesthesia? Anesth Analg 2000; 91:871–5Shao, X Li, H White, PF Klein, KW Kulstad, C Owens, A
- Singh H, Sakai T, Matsuki A: Movement response to skin incision: Analgesia vs. bispectral index and 95% spectral edge frequency. Eur J Anaesthesiol 1999; 16:610–4Singh, H Sakai, T Matsuki, A
- Sleigh JW, Donovan J: Comparison of bispectral index, 95% spectral edge frequency and approximate entropy of the, EEG, with changes in heart rate variability during induction of general anaesthesia. Br J Anaesth 1999; 82:666–71Sleigh, JW Donovan, J
- Sun R, Watcha MF, White PF, Skrivanek GD, Griffin JD, Stool L, Murphy MT: A cost comparison of methohexital and propofol for ambulatory anesthesia. Anesth Analg 1999; 89:311–6Sun, R Watcha, MF White, PF Skrivanek, GD Griffin, JD Stool, L Murphy, MT
- Vernon JM, Lang E, Sebel PS, Manberg P: Prediction of movement using bispectral electroencephalographic analysis during propofol/alfentanil or isoflurane/alfentanil anesthesia. Anesth Analg 1995; 80:780–5Vernon, JM Lang, E Sebel, PS Manberg, P
- White PF, Wang B, Tang J, Wender RH, Naruse R, Sloninsky A: The effect of intraoperative use of esmolol and nicardipine on recovery after ambulatory surgery. Anesth Analg 2003; 97:1633–8White, PF Wang, B Tang, J Wender, RH Naruse, R Sloninsky, A
- Wuesten R, Van Aken H, Glass PS, Buerkle H: Assessment of depth of anesthesia and postoperative respiratory recovery after remifentanil- versus alfentanil-based total intravenous anesthesia in patients undergoing ear–nose–throat surgery. Anesthesiology 2001; 94:211–7Wuesten, R Van Aken, H Glass, PS Buerkle, H
- Chazot T, Liu N, Tremelot L, Joukovsky P, Fischler M: Detection of gas embolism by Bispectral Index and entropy monitoring in two cases. Anesthesiology 2004; 101:1053–4Chazot, T Liu, N Tremelot, L Joukovsky, P Fischler, M
- Hayashida M, Chinzei M, Komatsu K, Yamamoto H, Tamai H, Orii R, Hanaoka K, Murakami A: Detection of cerebral hypoperfusion with bispectral index during paediatric cardiac surgery. Br J Anaesth 2003; 90:694–8Hayashida, M Chinzei, M Komatsu, K Yamamoto, H Tamai, H Orii, R Hanaoka, K Murakami, A
- Honan DM, Breen PJ, Boylan JF, McDonald NJ, Egan TD: Decrease in Bispectral Index preceding intraoperative hemodynamic crisis: Evidence of acute alteration of propofol pharmacokinetics. Anesthesiology 2002; 97:1303–5Honan, DM Breen, PJ Boylan, JF McDonald, NJ Egan, TD
- Kakinohana M, Miyata Y, Kawabata T, Kawashima S, Tokumine J, Sugahara K: Bispectral Index decreased to “0” in propofol anesthesia after a cross-clamping of descending thoracic aorta. Anesthesiology 2003; 99:1223–5Kakinohana, M Miyata, Y Kawabata, T Kawashima, S Tokumine, J Sugahara, K
- Kin N, Konstadt S, Sato K, Hanaoka K: Reduction of bispectral index value associated with clinically significant cerebral air embolism. J Cardiothorac Vasc Anesth 2004; 18:82–4Kin, N Konstadt, S Sato, K Hanaoka, K
- Luginbuhl M, Schnider TW: Detection of awareness with the Bispectral Index: Two case reports. Anesthesiology 2002; 96:241–3Luginbuhl, M Schnider, TW
- Merat S, Levecque J, Le Gulluche Y, Diraison Y, Brinquin L, Hoffmann J: BIS monitoring may allow the detection of severe cerebral ischemia. Can J Anesth 2001; 48:1066–9Merat, S Levecque, J Le Gulluche, Y Diraison, Y Brinquin, L Hoffmann, J
- Mourisse J, Booij L: Bispectral index detects period of cerebral hypoperfusion during cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2003; 17:76–8Mourisse, J Booij, L
- Welsby IJ, Ryan JM, Booth JV, Flanagan E, Messier RH, Borel CO: The bispectral index in the diagnosis of perioperative stroke: A case report and discussion. Anesth Analg 2003; 96:435–7Welsby, IJ Ryan, JM Booth, JV Flanagan, E Messier, RH Borel, CO
- Bruhn J, Bouillon TW, Shafer SL: Electromyographic activity falsely elevates the Bispectral Index. Anesthesiology 2000; 92:1485–7Bruhn, J Bouillon, TW Shafer, SL
- Gallagher JD: Pacer-induced artifact in the Bispectral Index during cardiac surgery. Anesthesiology 1999; 90:636Gallagher, JD
- Hemmerling TM, Desrosiers M: Interference of electromagnetic operating systems in otorhinolaryngology surgery with bispectral index monitoring. Anesth Analg 2003; 96:1698–9Hemmerling, TM Desrosiers, M
- Hemmerling TM, Fortier JD: Falsely increased bispectral index values in a series of patients undergoing cardiac surgery using forced-air-warming therapy of the head. Anesth Analg 2002; 95:322–3Hemmerling, TM Fortier, JD
- Hemmerling TM, Migneault B: Falsely increased bispectral index during endoscopic shoulder surgery attributed to interferences with the endoscopic shaver device. Anesth Analg 2002; 95:1678–9Hemmerling, TM Migneault, B
- Morimoto Y, Matsumoto A, Koizumi Y, Gohara T, Sakabe T, Hagihira S: Changes in the bispectral index during intraabdominal irrigation in patients anesthetized with nitrous oxide and sevoflurane. Anesth Analg 2005; 100:1370–4Morimoto, Y Matsumoto, A Koizumi, Y Gohara, T Sakabe, T Hagihira, S
- Mychaskiw G, Heath BJ, Eichhorn JH: Falsely elevated bispectral index during deep hypothermic circulatory arrest. Br J Anaesth 2000; 85:798–800Mychaskiw, G Heath, BJ Eichhorn, JH
- Myles PS, Cairo S: Artifact in the bispectral index in a patient with severe ischemic brain injury. Anesth Analg 2004; 98:706–7Myles, PS Cairo, S
- Puri GD, Bagchi A, Anandamurthy B, Dhaliwal RS: The Bispectral index and induced hypothermia–electrocerebral silence at an unusually high temperature. Anaesth Intensive Care 2003; 31:578–80Puri, GD Bagchi, A Anandamurthy, B Dhaliwal, RS
- Mychaskiw G II, Horowitz M, Sachdev V, Heath BJ: Explicit intraoperative recall at a bispectral index of 47. Anesth Analg 2001; 92:808–9Mychaskiw, G Horowitz, M Sachdev, V Heath, BJ
- Rampersad SE, Mulroy MF: A case of awareness despite an “adequate depth of anesthesia” as indicated by a bispectral index monitor. Anesth Analg 2005; 100:1363–4Rampersad, SE Mulroy, MF
- Chinzei M, Sawamura S, Hayashida M, Kitamura T, Tamai H, Hanaoka K: Change in bispectral index during epileptiform electrical activity under sevoflurane anesthesia in a patient with epilepsy. Anesth Analg 2004; 98:1734–6Chinzei, M Sawamura, S Hayashida, M Kitamura, T Tamai, H Hanaoka, K
- Hagihira S, Okitsu K, Kawaguchi M: Unusually low bispectral index values during emergence from anesthesia. Anesth Analg 2004; 98:10368Hagihira, S Okitsu, K Kawaguchi, M
- Schnider TW, Luginbuhl M, Petersen-Felix S, Mathis J: Unreasonably low Bispectral Index values in a volunteer with genetically determined low-voltage electroencephalographic signal. Anesthesiology 1998; 89:1607–8Schnider, TW Luginbuhl, M Petersen-Felix, S Mathis, J
- Viertio-Oja H, Maja V, Sarkela M, Talja P, Tenkanen N, Tolvanen-Laakso H, Paloheimo M, Vakkuri A, Yli-Hankala A, Merilainen P: Description of the entropy algorithm as applied in the Datex-Ohmeda S/5 Entropy Module. Acta Anaesth Scand 2004; 48:154–61Viertio-Oja, H Maja, V Sarkela, M Talja, P Tenkanen, N Tolvanen-Laakso, H Paloheimo, M Vakkuri, A Yli-Hankala, A Merilainen, P
- Vakkuri A, Yli-Hankala A, Sandin R, Mustola S, Høymork S, Nyblom S, Talja P, Sampson T, van Gils M, Viertiö-Oja H: Spectral entropy monitoring is associated with reduced propofol use and faster emergence in propofol–nitrous oxide–alfentanil anesthesia. Anesthesiology 2005; 103:274–9Vakkuri, A Yli-Hankala, A Sandin, R Mustola, S Høymork, S Nyblom, S Talja, P Sampson, T van Gils, M Viertiö-Oja, H
- Bruhn J, Bouillon TW, Radulescu L, Hoeft A, Bertaccini E, Shafer SL: Correlation of approximate entropy, Bispectral Index, and spectral edge frequency 95 (SEF95) with clinical signs of “anesthetic depth” during coadministration of propofol and remifentanil. Anesthesiology 2003; 98:621–7Bruhn, J Bouillon, TW Radulescu, L Hoeft, A Bertaccini, E Shafer, SL
- Vanluchene ALG, Struys MMRF, Heyse BEK, Mortier EP: Spectral entropy measurement during propofol and remifentanil: A comparison with the bispectral index. Br J Anaesth 2004; 93:645–54Vanluchene, ALG Struys, MMRF Heyse, BEK Mortier, EP
- Anderson RE, Barr G, Owell A, Jakobsson J: Entropy during propofol hypnosis including an episode of wakefulness. Anaesthesia 2004; 59:52–6Anderson, RE Barr, G Owell, A Jakobsson, J
- Wheeler PJ, Baughman VL, Koenig HM, Hoffman WE: The role of facial, EMG, and entropy EEG in evaluating adequacy of anesthesia. J Neurosurg Anesthesiol 2004; 16:373–4Wheeler, PJ Baughman, VL Koenig, HM Hoffman, WE
- Schultz B, Schultz A, Grouven U: Sleeping stage based systems (Narcotrend), New Aspects of High Technology in Medicine 2000. Edited by Bruch HP, Kockerling F, Bouchard R, Schug-Pab C. Bolognia, Monduzzi Editore, pp 285–91Schultz, B Schultz, A Grouven, U Bruch HP, Kockerling F, Bouchard R, Schug-Pab C. Bolognia, Monduzzi
- Chen X, Tang J, White PF, Wender RH, Ma H, Sloninsky A, Kariger R: A comparison of patient state index and bispectral index values during the perioperative period. Anesth Analg 2002; 95:1669–74Chen, X Tang, J White, PF Wender, RH Ma, H Sloninsky, A Kariger, R
- Wong CA, Fragen RJ, Fitzgerald PC, McCarthy RJ,: The association between propofol-induced loss of consciousness and the SNAPTMindex. Anesth Analg 2005; 100:141–8Wong, CA Fragen, RJ Fitzgerald, PC McCarthy, RJ
- Thornton C, Konieczko KM, Jones JG, Jordan C, Dore CJ, Heneghan CPH: Effect of surgical stimulation on the auditory evoked response. Br J Anaesth 1988; 60:372–8Thornton, C Konieczko, KM Jones, JG Jordan, C Dore, CJ Heneghan, CPH
- Kenny GN, Mantzaridis H: Closed-loop control of propofol anaesthesia. Br J Anaesth 1999; 83:223–8Kenny, GN Mantzaridis, H
- Schwender D, Conzen P, Klasing S, Finsterer U, Poppel E, Peter K: The effects of anesthesia with increasing end-expiratory concentrations of sevoflurane on midlatency auditory evoked potentials. Anesth Analg 1995; 81:817–22Schwender, D Conzen, P Klasing, S Finsterer, U Poppel, E Peter, K
- Maattanen H, Anderson R, Uusijarvi J, Jakobsson J: Auditory evoked potential monitoring with the AAI™-index during spinal surgery: Decreased desflurane consumption. Acta Anaesthesiol Scand 2002; 46:882–6Maattanen, H Anderson, R Uusijarvi, J Jakobsson, J
- Muncaster AR, Sleigh JW, Williams M: Changes in consciousness, conceptual memory, and quantitative electroencephalographical measures during recovery from sevoflurane- and remifentanil-based anesthesia. Anesth Analg 2003; 96:720–5Muncaster, AR Sleigh, JW Williams, M
- Doi M, Gajra RJ, Mantzaridis H, Kenny GN: Prediction of movement at laryngeal mask airway insertion: Comparison of auditory evoked potential index, bispectral index, spectral edge frequency and median frequency. Br J Anaesth 1999; 82:203–7Doi, M Gajra, RJ Mantzaridis, H Kenny, GN
- Weber F, Bein T, Hogghahn J, Taeger K: Evaluation of the Alaris auditory evoked potential index as an indicator of anesthetic depth in preschool children during induction of anesthesia with sevoflurane and remifentanil. Anesthesiology 2004; 101:294–8Weber, F Bein, T Hogghahn, J Taeger, K
- Gajraj RJ, Doi M, Mantzaridis H, Kenny GN: Analysis of the EEG bispectrum, auditory evoked potentials and the EEG power spectrum during repeated transitions from consciousness to unconsciousness. Br J Anaesth 1998; 80:46–52Gajraj, RJ Doi, M Mantzaridis, H Kenny, GN
- Ge SJ, Zhuang XL, Wang YT, Wang ZD, Chen SL, Li HT: Performance of the rapidly extracted auditory evoked potentials index to detect the recovery and loss of wakefulness in anesthetized and paralyzed patients. Acta Anaesth Scand 2003; 47:466–71Ge, SJ Zhuang, XL Wang, YT Wang, ZD Chen, SL Li, HT
- Monk TG, Saini V, Weldon BC, Sigl JC: Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg 2005; 100:4–10Monk, TG Saini, V Weldon, BC Sigl, JC
- Enlund M, Hassan HG: Intraoperative awareness: Detected by the structured Brice interview? Acta Anaesthesiol Scand 2002; 46:345–9Enlund, M Hassan, HG
- Famewo CE: Awareness and dreams during general anaesthesia for Caesarian section a study of incidence. Can Anaesth Soc J 1976; 23:636–9Famewo, CE
- Ho AM: ‘Awareness’ and ‘recall’ during emergence from general anaesthesia. Eur J Anaesth 2001; 18:623–5Ho, AM
- Munte S, Schmidt M, Meyer M, Nager W, Lullwitz E, Munte TF, Piepenbrock S: Implicit memory for words played during isoflurane- or propofol-based anesthesia: The lexical decision task. Anesthesiology 2002; 96:588–94Munte, S Schmidt, M Meyer, M Nager, W Lullwitz, E Munte, TF Piepenbrock, S
- Wennervirta J, Ranta SO, Hynynen M: Awareness and recall in outpatient anesthesia. Anesth Analg 2002; 95:72–7Wennervirta, J Ranta, SO Hynynen, M
Appendix 1: Summary of Practice Advisory
Preoperative Evaluation
- Review patient medical records for potential risk factors
- - Substance use or abuse
- - Previous episode of intraoperative awareness
- - History of difficult intubation or anticipated difficult intubation
- - Chronic pain patients using high doses of opioids
- - ASA physical status IV or V
- - Limited hemodynamic reserve
- Interview patient
- - Assess level of anxiety
- - Obtain information regarding previous experiences with anesthesia
- Determine other potential risk factors
- - Cardiac surgery
- - Cesarean delivery
- - Trauma surgery
- - Emergency surgery
- - Reduced anesthetic doses in the presence of paralysis
- - Planned use of muscle relaxants during the maintenance phase of general anesthesia
- - Planned use of nitrous oxide–opioid anesthesia
- Patients whom the individual clinician considers to be at substantially increased risk of intraoperative awareness should be informed of the possibility of intraoperative awareness when circumstances permit
Preinduction Phase of Anesthesia
- Adhere to a checklist protocol for anesthesia machines and equipment to assure that the desired anesthetic drugs and doses will be delivered
- Verify the proper functioning of intravenous access, infusion pumps, and their connections, including the presence of appropriate backflow check valves
- The decision to administer a benzodiazepine prophylactically should be made on a case-by-case basis for selected patients (e.g. , patients requiring smaller dosages of anesthetics)
Intraoperative Monitoring
- Use multiple modalities to monitor depth of anesthesia
- - Clinical techniques (i.e. , checking for purposeful or reflex movement)
- ▪ Neuromuscular blocking drugs may mask purposeful or reflex movement
- - Conventional monitoring systems (e.g. , electrocardiogram, blood pressure, heart rate, end-tidal anesthetic analyzer, capnography)
- - Brain function monitoring
- ▪ Not routinely indicated for general anesthesia patients
- ▪ The decision to use a brain function monitor should be made on a case-by-case basis by the individual practitioner for selected patients (e.g. , light anesthesia)
Intraoperative and Postoperative Management
- The decision to administer a benzodiazepine intraoperatively after a patient unexpectedly becomes conscious should be made on a case-by-case basis
- Speak with patients who report recall of intraoperative events to obtain details of the event and to discuss possible reasons for its occurrence
- A questionnaire or structured interview may be used to obtain a detailed account of the patient’s experience
- Once an episode of intraoperative awareness has been reported, an occurrence report regarding the event should be completed for the purpose of quality management
- Offer counseling or psychological support to those patients who report an episode of intraoperative awareness
Appendix 2: Literature Review and Consensus-based Evidence
For this Advisory, a literature review was used in combination with opinions obtained from experts and other sources (e.g. , professional society members, open forums, Web-based postings) to provide guidance to practitioners regarding intraoperative awareness. Both the literature review and opinion data were based on evidence linkages , consisting of directional statements about relationships between specific perioperative interventions and intraoperative awareness. The evidence linkage interventions are listed below:
Preoperative Evaluation
- Focused history (i.e. , medical records, patient interview, physical examination)
- Patient characteristics associated with risk of awareness
- Procedures associated with higher risk of intraoperative awareness
- Anesthetic techniques associated with higher risk of intraoperative awareness
- Informing patients of the possibility of intraoperative awareness
Preinduction Phase of Anesthesia
- Check anesthesia delivery systems to reduce errors
- Prophylactic administration of benzodiazepines as coanesthetics
Intraoperative Monitoring
- Commonly used clinical techniques
- Conventional monitoring systems
- Brain function monitors
- - Spontaneous electrical activity (electroencephalograph/electromyograph)
- ▪ Bispectral Index
- ▪ Danmeter Cerebral State Monitor/Cerebral State Index
- ▪ Entropy
- ▪ Narcotrend®
- ▪ Patient state analyzer
- ▪ SNAP index
- - Evoked electrical activity (auditory evoked potential monitoring)
- ▪ AEP Monitor/2
Intraoperative and Postoperative Interventions
- Intraoperative use of benzodiazepines for unexpected consciousness
- Structured interview of patients who report recall of intraoperative events
- Questionnaire administered to patients who report recall of intraoperative events
- Patient counseling for patients who report recall of intraoperative events
State of the Literature
A study or report that appears in the published literature is included in the development of an advisory if the study (1) is related to one of the specified linkage statements, (2) reports a finding or set of findings that can be tallied or measured (e.g. , articles that contain only opinion are not included), and (3) is the product of an original investigation or report (i.e. , review articles or follow-up studies that summarize previous findings are not included).
For the literature review, potentially relevant studies were identified via electronic and manual searches of the literature. The electronic search covered a 40-yr period from 1966 through 2005. The manual search covered a 36-yr period of time from 1970 through 2005. More than 1,500 citations were initially identified, yielding a total of 711 nonoverlapping articles that addressed topics related to the evidence linkages and met our criteria for inclusion. After review of the articles, 389 studies did not provide direct evidence and were subsequently eliminated. A total of 322 articles contained direct linkage-related evidence. No evidence linkage contained enough studies with well-defined experimental designs and statistical information to conduct a quantitative analysis (i.e. , meta-analysis).
Interobserver agreement among Task Force members and two methodologists was established by interrater reliability testing. Agreement levels using a κ statistic for two-rater agreement pairs were as follows: (1) type of study design, κ= 0.60–0.85; (2) type of analysis, κ= 0.60–0.93; (3) evidence linkage assignment, κ= 0.77–0.88; and (4) literature inclusion for database, κ= 0.76–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav = 0.82, Var (Sav) = 0.007; (2) type of analysis, Sav = 0.73, Var (Sav) = 0.008; (3) linkage assignment, Sav = 0.69, Var (Sav) = 0.012; and (4) literature database inclusion, Sav = 0.84, Var (Sav) = 0.014. These values represent moderate to high levels of agreement.
The primary focus of this Advisory was to examine studies with hypothesis-driven research designs, such as RCTs, that examined the effect of an intervention (such as a brain function monitor) on reducing the occurrence or frequency of intraoperative awareness. To date, only two randomized controlled trials were found that reported intraoperative awareness as the primary study endpoint.55,56 Additional controlled trials will be necessary before data from published literature can be aggregated to provide a basis for quantitative evidence (i.e. , meta-analysis).
Several other RCTs were reviewed that reported primary outcomes other than intraoperative awareness, including emergence time, consumption of anesthetic drugs, and recovery characteristics. In addition, many other published studies applied non–hypothesis-driven research designs to obtain noncausal or indirect data. For example, descriptive literature (i.e. , reports of frequency or incidence) may provide an indication of the scope of the problem. Correlational or predictive data provide information regarding the direction and strength of association of values obtained from patient monitoring devices with other intraoperative measures such as blood concentrations of anesthetic drugs, time to loss of eyelash reflex, and time to awakening. Case reports are typically used as a forum for reporting and recognizing unusual or unintended benefits or harms. Often, case reports as well as descriptive or correlational data provide useful hypotheses-generating information that may stimulate additional causal examination of the topic of intraoperative awareness.
Future studies should focus on prospective methodologies, when possible, that use traditional hypothesis testing techniques. Use of the following methodologic procedures for assessing the impact of interventions for intraoperative awareness is recommended: (1) comparison studies assessing the efficacy of one technique versus other techniques; (2) random assignment to treatment groups with blinding if appropriate; and (3) full reporting of sample size, effect size estimates, test scores, measures of variability, and P values. The Task Force recognizes that, because intraoperative awareness is a very-low-incidence event, conducting such studies may be difficult and expensive. The required sample size for a RCT to test the impact of an intervention (e.g. , brain function monitor) on the incidence of intraoperative awareness is invariably large. The Task Force also recognizes that, with low-incidence data, a difference in the recording of one or two cases of intraoperative awareness can affect the statistical significance of study findings.
Limiting the study to patient subgroups thought to have a higher risk for intraoperative awareness (e.g. , cardiac surgery, cesarean delivery, emergency trauma surgery) may allow for a smaller sample size and provide useful information regarding these subgroups. However, the Task Force recognizes that the generalizability of these findings to the larger population of general anesthesia patients may be limited.
Consensus-based Evidence
Consensus was obtained from multiple sources, including (1) survey opinion from consultants who were selected based on their knowledge or expertise in intraoperative awareness, (2) survey opinions from a randomly selected sample of active members of the ASA, (3) testimony from attendees of three open forums held at national anesthesia meetings,5(4) Internet commentary, and (5) Task Force opinion and interpretation. The survey rate of return was 60% (n = 57 of 95) for consultants and 30% (n = 151/500) for the ASA membership. Survey results are presented in the text of the document and in tables 1 and 2.

Table 1
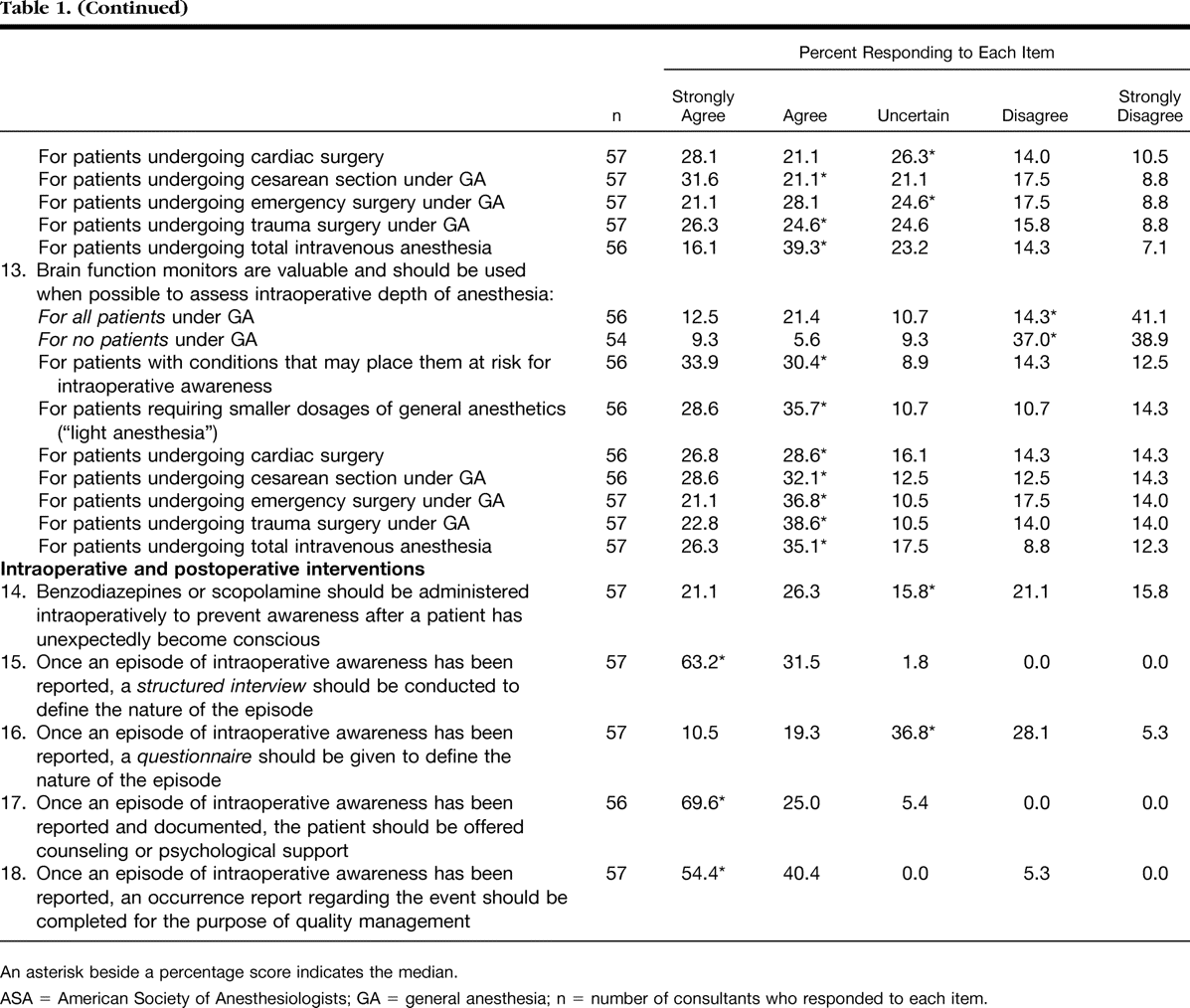
Table 1(continued)

Table 2

Table 2 (continued)
Ninety-one percent of the consultants and 72% of the ASA members indicated that they had personally used a brain function device in the past. Fifty-seven percent of the consultants indicated that they make use in their current practice of a brain function device always (11.1%), frequently (20.4%), or sometimes (25.9%). Thirty-six percent of the ASA members indicated that they make use in their current practice of a brain function device always (6.0%), frequently (13.4%), or sometimes (16.8%).
The consultants were also asked to indicate which, if any, of the evidence linkages would change their clinical practices if the Advisory was instituted. The rate of return was 18% (n = 17 of 95). The percent of responding consultants expecting no change associated with each linkage were as follows: preoperative evaluation—82%; informing patients of the possibility of intraoperative awareness—65%; check anesthesia delivery systems—94%; prophylactic use of benzodiazepines as coenesthetics—100%; use of clinical techniques to monitor for intraoperative awareness—94%; use of conventional monitoring systems to monitor for intraoperative awareness—100%; use of brain function monitors to monitor for intraoperative awareness—59%; intraoperative use of benzodiazepines for unexpected consciousness—100%; use of a structured interview for patients who report recall of intraoperative events—41%; use of a questionnaire for patients who report recall of intraoperative events—53%; and counseling for patients who report recall of intraoperative events—76%. Seventy-one percent of the respondents indicated that the Advisory would have no effect on the amount of time spent on a typical case. Four respondents (24%) indicated that there would be an increase in the amount of time they would spend on a typical case with the implementation of this Advisory. The amount of increased time anticipated by these respondents ranged from 1 to 20 min.


