Surgical Site Infection Reduction
Surgical Site Infection Reduction

To help reduce surgical site infections, cardiac surgery (CS) programs should include a care bundle that includes topical intranasal therapies, depilation protocols, and appropriate timing and stewardship of perioperative prophylactic antibiotics, combined with smoking cessation, adequate glycemic control, and promotion of postoperative normothermia during recovery. Moderate-quality meta-analysis have concluded that care bundles of 3 to 5 evidence-based interventions can reduce surgical site infections. This topic has been reviewed extensively with class of recommendation and level of evidence in an expert consensus review by Lazar et al.
Evidence supports topical intranasal therapies to eradicate staphylococcal colonization in patients undergoing CS. From 18% to 30% of all patients undergoing surgery are carriers of Staphylococcus aureus, and they have 3 times the risk of S. aureus surgical site infections and bacteremia. It is recommended that topical therapy be applied universally. Two studies validate the reduction of such infections in patients receiving mupirocin. Level IA data exists suggesting that weight-based cephalosporins should be administered fewer than 60 minutes before the skin incision and continued for 48 hours after completion of CS. When the surgery is more than 4 hours, antibiotics require redosing. Clarity on the preferability of continuous vs intermittent dosing of cefazolin requires further data. A meta-analysis of skin preparation and depilation protocols indicates that clipping is preferred to shaving. Clipping using electric clippers should occur close to the time of surgery. A preoperative shower with chlorhexidine has only been demonstrated to reduce bacterial counts in the wound and is not associated with significant levels of efficacy. Postoperative measures including sterile dressing removal within 48 hours and daily incision washing with chlorhexidine are potentially beneficial.
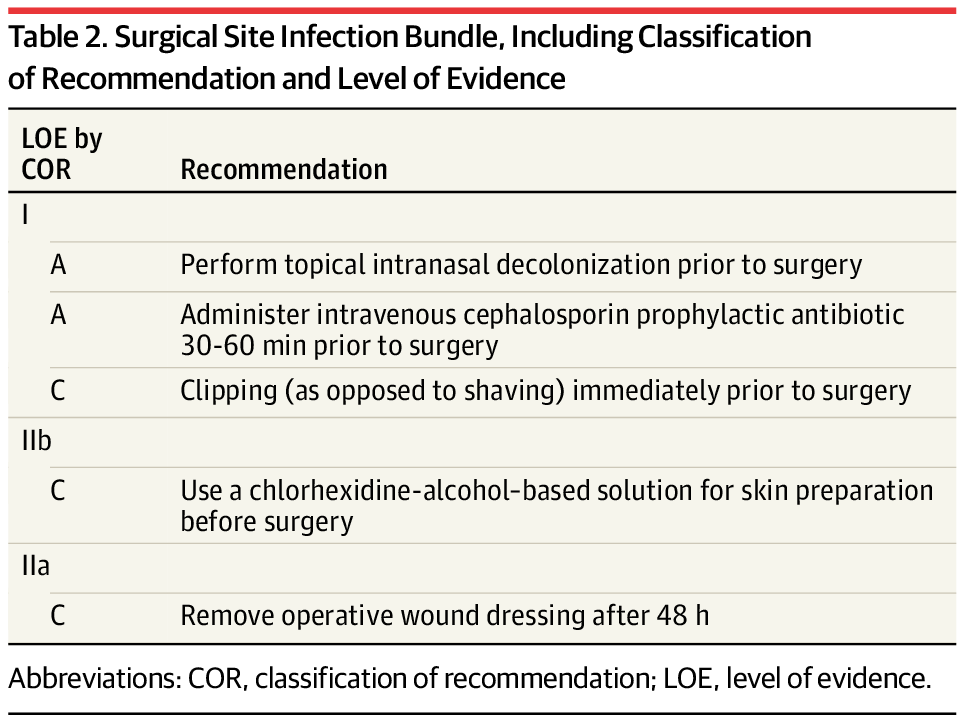
In summary, we recommend the implementation of a care bundle to include topical intranasal therapies to eradicate staphylococcal colonization, weight-based cephalosporin infusion fewer than 60 minutes before skin incision, with redosing for cases longer than 4 hours, skin preparation, and depilation protocols with dressing changes every 48 hours to reduce surgical site infections (class I, level B-R). The bundle of recommendations to reduce surgical site infections is summarized in Table below with the classification of recommendations and level of evidence per Lazar et al.
source: jama


